We’ve been hearing quite a lot about The Science these days. So, what is science? How does science guide medical practice and naturopathic medicine?
The science council defines science as, “the pursuit and application of knowledge and understanding of the natural and social world following a systematic methodology based on evidence.” The answer is, science is a methodology.
It is applied in medicine through Evidence Based Medicine (EBM) which starts with the individual patient and incorporates: clinical expertise, scientific evidence (that best that exists according to a hierarchy), and patient values and preferences.
“Evidence medicine is the conscientious, explicit, judicious and reasonable use of modern, best evidence in making decisions about the care of individual patients. EBM integrates clinical experience and patient values with the best available research information.”
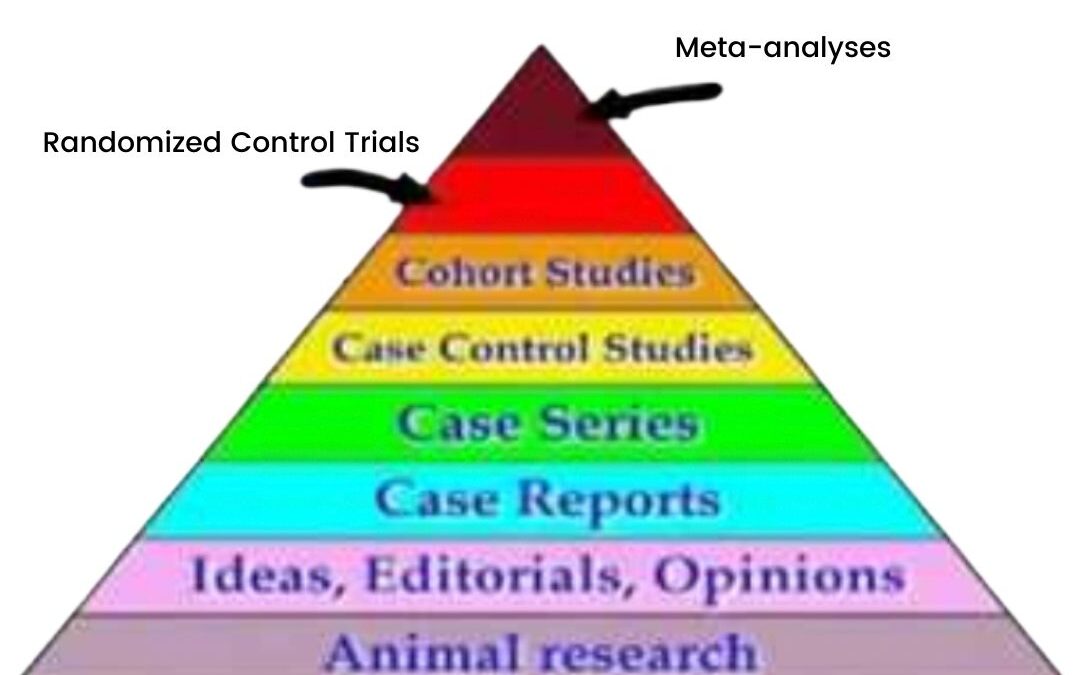
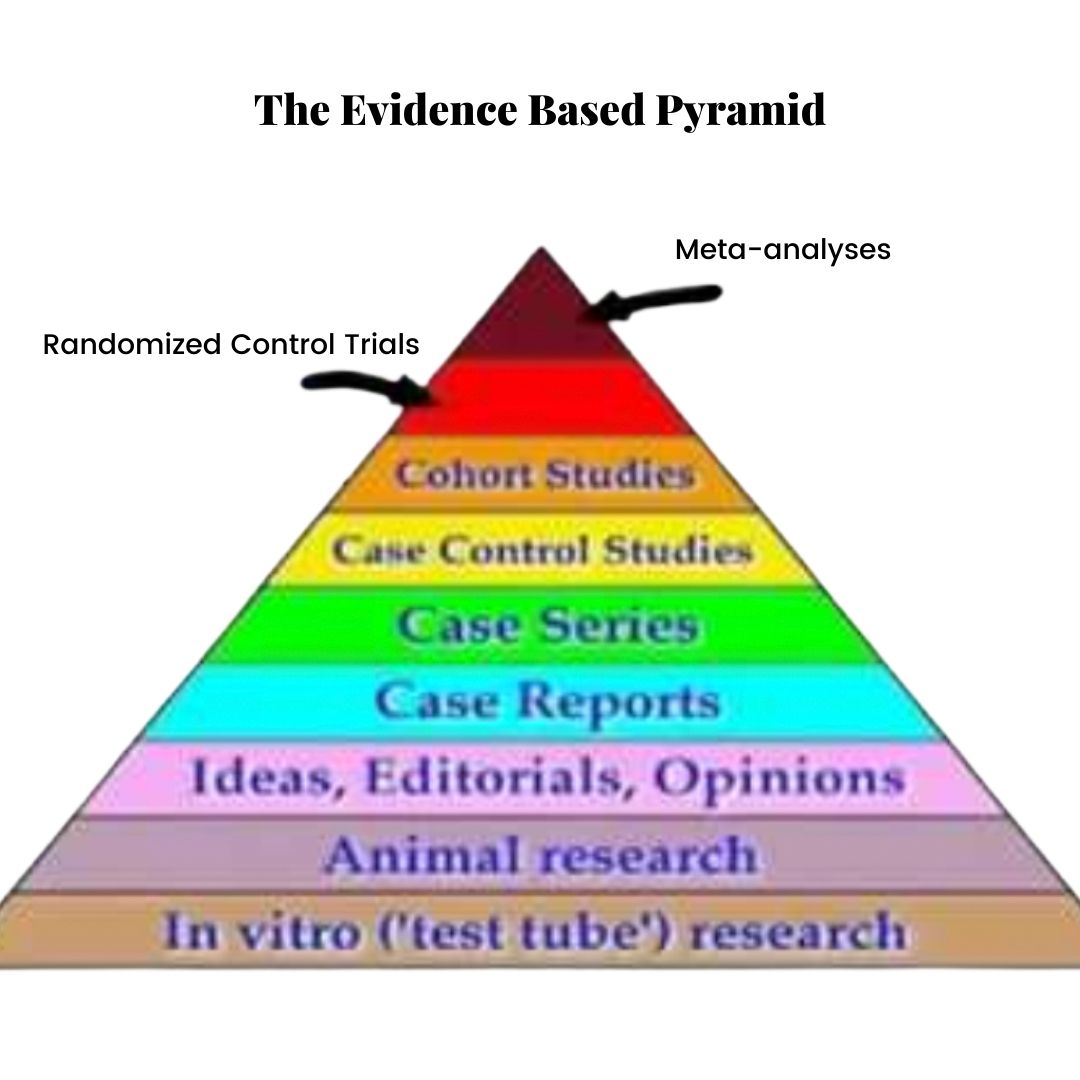
The Evidence-Based Pyramid
In EBM, evidence exists in a hierarchy, represented by the Evidence Based Pyramid (shown above). Animal studies are at the bottom, case reports (clinical anecdotes) somewhere in the middle and randomized control trials and meta-analyses (the Gold Standard of evidence) at the top.
Dave Sackett (the Father of EBM) et al. write in the British Medical Journal (1996),
“Good doctors use both individual clinical expertise and the best available external evidence and neither alone is enough.”
In addiction to scientific evidence, EBM must incorporate:
Patient values
A bottom-up approach (it is patient-centred, not guideline-centred)
The needs of the individual (EBM is not a one-size-fits-all formula)
Clinical expertise
The best available evidence: this does not mean using only randomized control trials. Sometimes the best evidence we have are case reports, historical and traditional use of an herb or animal studies. We still owe our patients the opportunity to see if a treatment works for them, especially if the risk of a given treatment is low.
As clinicians, we use our knowledge in different ways. We start with an assessment of the individual in front of us. This assessment takes into account the factors that influence this patient’s life, their lifestyle, their health condition and their overall health goals.
We then turn to clinical experience, research, our scientific knowledge and guidelines.
We share this information with our patient. Our job is to educate and convey the options so that the individual can provide informed consent. How does this knowledge fit into the patient’s life? How does it inform their choice?
Science is not a set of values. It is not a religion. We do not follow it.
Science provides us with a methodology for seeking the answers to questions we might ask about how the principles of nature, including the human body, are organized.
Science encourages us to ask questions and testing hypotheses in order to find answers.
It is never settled.
Most of all, science doesn’t tell us how to use scientific knowledge.
Our choices are governed by our goals, preferences and values.
So, “follow the sicence?”
No. Follow your goals, preferences, values and dreams.
And use science to help guide your way.
Reference:
Sackett, D. L., Rosenberg, W. C., Gray, J. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. BMJ, 312(7023), 71–72.
“There exists in such a case a certain institution or law; let us say, for the sake of simplicity, a fence or gate erected across a road. The more modern type of reformer goes gaily up to it and says, “I don’t see the use of this; let us clear it away.” To which the more intelligent type of reformer will do well to answer: “If you don’t see the use of it, I certainly won’t let you clear it away. Go away and think. Then, when you can come back and tell me that you do see the use of it, I may allow you to destroy it.”
In other words, beware of tearing down structures until you fully understand their benefit.
Chesterton’s Fence can also be thought of as the Precautionary Principle. Not following this principle led to scientific practices like frontal lobotomies or removing the entire large intestine because doctors didn’t understand the benefits of these structures or the consequences of removing them.
A narrow range of focus, i.e., this organ is causing a problem, or we don’t know why it’s here, led to drastic action that resulted in unforeseen, disastrous consequences.
I believe that such is the case with our stomach acid.
The stomach is essentially a lined bag filled with acid. Stomach pH is from 1.5 to 3.5, acidic enough to burn a hole in your shoe. However, the mucus layer of the stomach protects it from being destroyed by the acid. The acid in the stomach helps dissolve and digest the food chewed up by the teeth and swallowed.
Stomach pH is needed for breaking down proteins. Stomach acid also plays a role in absorbing minerals such as calcium, zinc, manganese, magnesium, copper, phosphorus and iron. It activates intrinsic factor, which is needed for B12 absorption in the small intestine.
Stomach acid regulates the rate of gastric emptying, preventing acid reflux.
Fast-forward to a condition called gastric esophageal reflux disease, or GERD. GERD affects about 20% of Western countries, characterized by high esophageal pH and reflux of the stomach acid and stomach contents into the esophagus. While the stomach is designed to handle a shallow pH environment, the esophagus is not. A doorway called the lower esophageal sphincter, or LES, keeps stomach contents where they should be–in the stomach.
In GERD, the tone of the LES is weak, resulting in a backflow of stomach contents. This can damage the esophagus, causing heartburn, pain, bad breath, coughing and even problems like ear pain, sore throat, and mucus in the throat. Silent reflux occurs when these symptoms occur without burning.
The symptoms occur from the stomach’s acidic contents irritating the more delicate tissues of the esophagus. So, rather than treat the root problem, i.e., the reflux, drugs like proton pump inhibitors (PPIs), H2 blockers, and buffers like Tums are recommended to reduce the stomach’s acidity.
Essentially, with GERD, we are tearing down Chesterton’s Fence to pave a road without taking even a moment to consider why the fence might be there in the first place.
About 12% of people are prescribed PPIs. They are given for GERD, gastritis, and IBS symptoms like bloating and stomach pain. Most of my patients are prescribed them for virtually any stomach complaint. PPIs, it seems, are the hammers wielded by many GPs, and so every digestive concern must look like a nail. Most people are put on them inevitably, without a plan to end the use and address the root cause of symptoms, which in most GERD cases are low LES tone.
PPIs raise stomach pH, disrupting stomach function. This causes issues with mineral absorption and protein digestion. Their use results in B12, vitamin C, calcium, iron, and magnesium deficiencies. Many of these deficiencies, like magnesium deficiency, can’t be tested and therefore might show up sub-clinically in tight muscles, headaches, painful periods, disrupted sleep and anxiety, and constipation. Therefore they fly under the radar of most primary care doctors.
No one connects someone’s heartburn medication with their recent onset of muscle tightness and anxiety.
Many of my patients report difficulties digesting meat and feeling bloated and tired after eating, particularly when consuming a protein-rich meal. They conclude that the meat isn’t good for them. The problem, however, is not meat but that stomach acid that is too diluted to break down the protein in their meal, leading to gas and bloating as the larger protein fragments enter the small intestine.
Many digestive problems result from this malabsorption and deficiency in stomach acid, not too much. Zinc is required for stomach acid production, and one of the best sources of zinc is red meat (zinc is notoriously lacking from plant foods). I have recently been prescribing lots of digestive enzymes and zinc to work my patients’ digestive gears.
Therefore, beware of tearing down a fence without understanding why it’s there. Stomach acid is essential for digesting our food, and regulating blood sugar and building muscle mass through protein digestion.
It is necessary for mineral absorption and B12 digestion. Our stomachs were designed to contain an extremely low pH. They evolved over millennia to do this. Stomach acid is low for a reason. It’s highly unlikely that our bodies made a mistake when it comes to stomach acid.
Therefore, beware of messing with it.
Consider that our bodies know what they’re doing. Consider the importance of finding and treating the actual root cause, not one factor that, if mitigated, can suppress symptoms while causing a host of other problems.
Don’t block your stomach acid.
As Hippocrates said, “All disease begins in the gut.”
It is the boundary between us and the outside world, the border where our body carefully navigates what can come in and nourish us and what should stay outside of us: our fence. Beware of tearing it down.
References:
Antunes C, Aleem A, Curtis SA. Gastroesophageal Reflux Disease. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441938/
Daniels B, Pearson SA, Buckley NA, Bruno C, Zoega H. Long-term use of proton-pump inhibitors: whole-of-population patterns in Australia 2013-2016. Therap Adv Gastroenterol. 2020;13:1756284820913743. Published 2020 Mar 19. doi:10.1177/1756284820913743
Heidelbaugh JJ. Proton pump inhibitors and risk of vitamin and mineral deficiency: evidence and clinical implications. Ther Adv Drug Saf. 2013;4(3):125-133. doi:10.1177/2042098613482484
A naturopathic doctor offers tips for navigating the often contradictory and confusing world of modern human nutrition.
As soon as we start to feel comfortable with our grasp of human nutrition—which foods are healthy, which ones are unhealthy, and how to eat a balanced diet for optimal health—a new study gets published that shatters our once-felt sense of confidence.
Confusingly contradictory health claims constantly appear in the news, like the American Heart Association’s vilification of coconut oil. The vegan diet-promoting documentary What the Health, currently trending on Netflix, turns convention on it head by assuaging our fears of refined sugar, instead blaming animal protein, eggs and dairy for the worldwide diabetes epidemic. Even I find myself doubting the 15 years I’ve spent studying and working in the field of human health every time paradoxical nutritional data is uncovered.
When I was in high school, I remember patting myself on the back for choosing fat-free options, hoping the leanness of my food would encourage leanness of my flesh. I gave up meat, understanding that I was making a healthier choice; I was told that meat, fat and cholesterol were all culprits of heart disease. I tried giving up eggs and dairy, trying on veganism in order to minimize my impact on the environment. I did an elimination diet while at naturopathic medical school, removing gluten. When my colleagues started reading about the Paleo Diet—grains were the enemy all along, while meat was good for us—I slowly began to embrace a “primal” diet. I started removing myself from the influence of decades’ worth of poorly conducted research and began welcoming saturated fat back into my life. Fat was fine; it was carbs that were the root of all disease. Atkins had gotten it right from the beginning. Eventually I cut out all carbs and sugar and tried a ketogenic diet, eating lots of fat, moderate amounts of meat, and some vegetables.
My journey brings me here, to my Facebook newsfeed, which has been infiltrated with articles condemning coconut oil and saturated fat for raising LDL cholesterol and contributing to cardiovascular disease. “But I thought it was healthy!” Friends, family and patients cry, tearing their hair out in confusion over the news. Some patients have watched Netflix’s What the Health, a documentary from the makers of Cowspiracy, which asserts that sugar’s link to type II diabetes may not bas as strong as previously thought.
The flip-flopping is frustrating for sure, especially for those of us who are committed to living healthy lives for as long as possible. But before we toss our tubs of coconut oil and liquid stevia drops in the garbage and start pulling out the white sugar and margarine again, we should consider how nutritional research is conducted. Let’s entertain different traditional, holistic viewpoints on food and nutrition in order to learn how to feed our bodies optimally.
The Problem with Nutritional Research
There are several problems with how we study nutrition. One of the challenges lies within science itself; scientific studies, by their very nature, attempt to isolate all of life’s complexity down to two variables in order to study them while nutrition, as it’s practised in the day to day lives of human beings, consists of an infinite number of important factors that are often not taken into account.
Most human diet studies are epidemiological. Researchers follow populations of people for years, tracking what they eat and noting how many diseases they get over time. They then synthesize the data to create story. For instance, how much fibre did the people who had heart disease eat? Did those who avoided gluten have a higher risk of diabetes?
In order to assess dietary intake, most epidemiological studies use Food Frequency Questionnaires, or FFQs. Study participants are asked how often they eat certain foods (such as chicken) per week. They are asked to check a box, from “none” to “more than 6 times a week”. As a clinician interested in how my patients’ nutrition may be affecting their health, I assess diet in a few different ways. In the initial appointment, I ask my patients to recall everything they’ve consumed in the past 24 hours to get a rough overview of how they typically eat. Then, between the first and second appointments, I have my patients track their foods in a diet diary over the course of one to two weeks. The accuracy with which my patients report their food intake from the day before depends on their memories, perceptions, and diligence in recording, among other things, and this can compare drastically with their diet diaries that are recorded in real time. Not only do the mundane memories of daily meals evade us, we are often found guilty of deceiving ourselves based on how we feel we should be eating, rather than how we actually are. I find it hard to believe that participants are filling out FFQs accurately.
Also, the stories that epidemiological studies create from the data establish correlation, not causation. With many correlations (like one of my favourites: ice cream consumption and drowning—both occur in summer) there is often no direct relationship. If assessing the connection between fat intake and diabetes, a good study will take into account all meaningful variables, such as how often the participants exercised, or whether they had existing cardiovascular disease. However, considering all the possible factors that might effect the relationship is virtually impossible. For instance, what was the status of the gut flora of the participants? What was their antioxidant or mineral status; were they magnesium deficient? Were they consuming meat that was pasture-raised or corn-fed? How high was their daily toxic exposure? Did they experience chronic stress? How well were they sleeping? What were their levels of inflammation like? And so on.
The trouble with studying nutrition and disease is that, when it comes to health, context matters; context may be all that matters. For instance, while we know that barbecued meat can produce carcinogens that potentially lead to cancer, a study found that when the meats were seasoned with rosemary the carcinogenic load of the meat was neutralized. It’s nearly impossible to form a complete picture when we insist on studying isolated factors, leaving out many important details.
Animal studies, while allowing for tighter control (we don’t ask mice to report their diets, we just feed them), are also flawed. Firstly, mice and humans are completely different species with different nutrient requirements. However, animal study designs can also be problematic. Animals are given lard and white sugar to assess the effects of a high fat, high sugar diet on their health—their diets are exaggerated for the purpose of the study. Human beings, however, eat burgers, cake, and ice cream. We don’t eat single nutrients like fat and sugar, we eat food. If a mouse gets sick on a diet of lard and table sugar is it because of the foods it was eating, something he wasn’t eating, or some other unforeseen factor? There may be a huge difference between eating a high-fat diet with no vitamins and minerals, and eating a high-fat diet that contains complete nutrition.
A third method for studying human nutrition is through randomized control trials, or RCTs. In RCTs humans are randomized into a group that receives an intervention, like a dietary plan, or a control group that is told to follow some other diet or just eat normally. These trials control as many variables as possible, but the timeframe for these studies is often too short to garner meaningful information about health outcomes, which may take years to manifest. It is also difficult to get participants to stick to meal plans. Further, it’s hard to establish consensus for each diet being studied. For example, when assessing the nutritional merits of the Paleo diet, how many servings of vegetables should participants be told to consume? How many grams of fat? What types of fat?
It’s important that we can use studies to seek answers to our questions about the relationship between nutrition and health. However, due to its many limitations, nutritional research can only take us so far. This is why one study may indicate that high sugar diets contribute to diabetes risk, while another study finds no relationship.
A New Food Guide
If we can’t trust research studies to tell us what to eat, who do we trust? Surely we can’t rely on Canada’s Food Guide, with it’s outdated recommendations that simultaneously overemphasize grains and dairy, while continuing to uphold archaic views on fat. Primarily created in the 40’s to help Canadian families ration their food during the war, the Food Guide was not necessarily created to promote the optimal health of those who follow it.
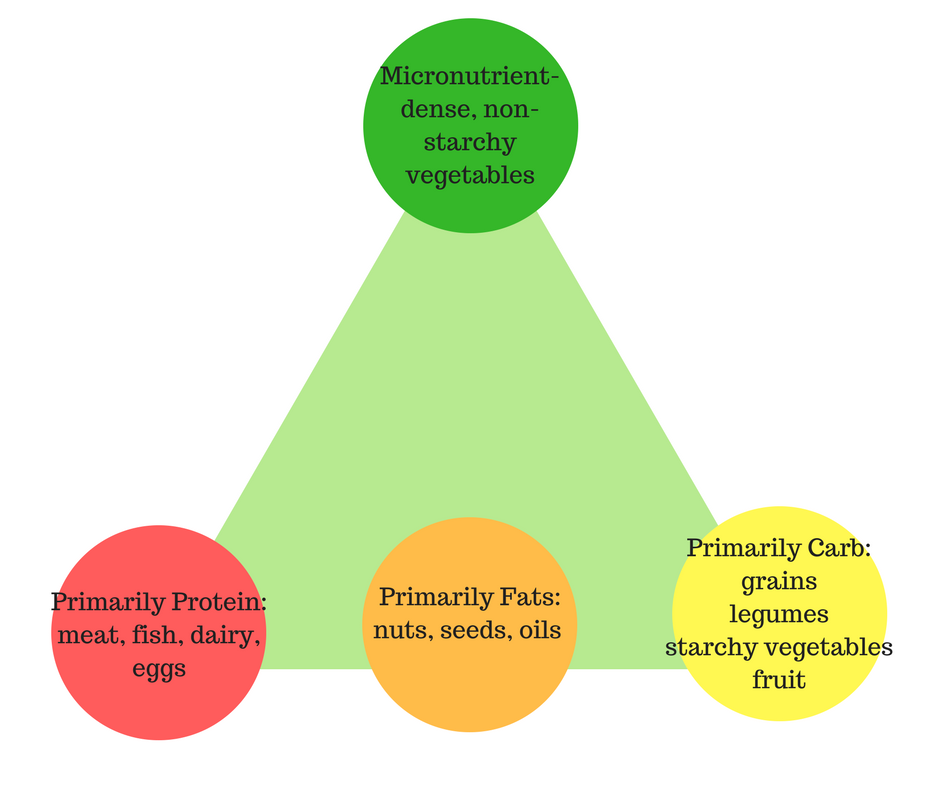
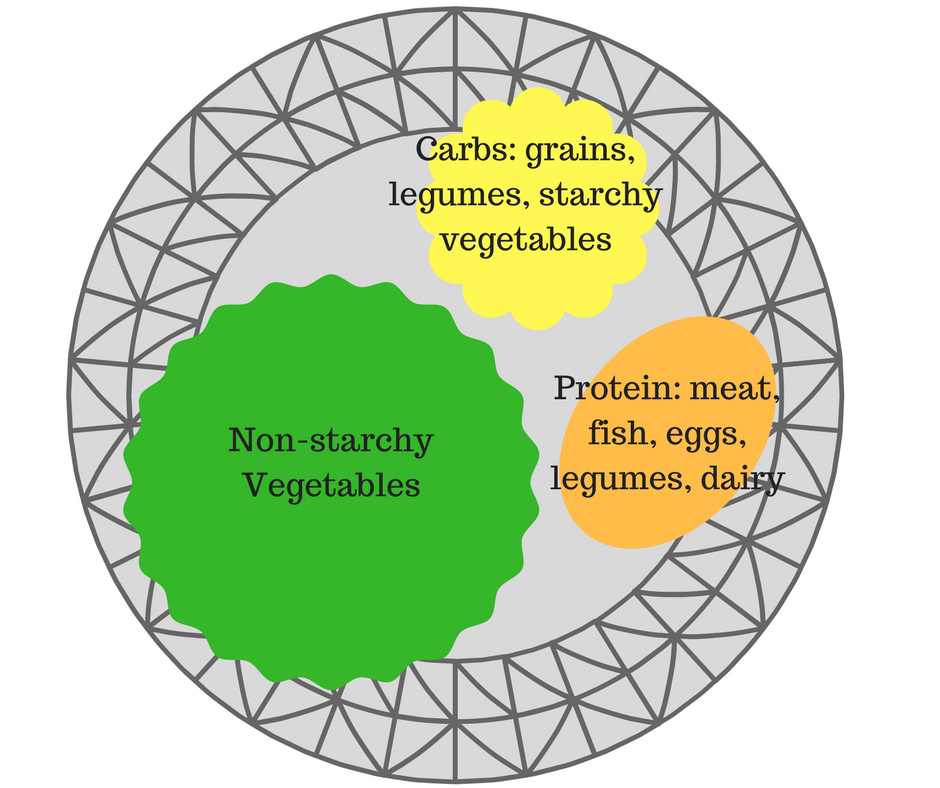
Dr. Ray Cronise, a former NASA scientist, outlines a food pyramid in his paper to help organize food into nutrient content. I often borrow his pyramid to depict nutritional balance to my patients.
Ray’s pyramid is composed of four circles, three that form the base of the pyramid, forming the three main groups of macronutrients: protein, fat, and carbohydrates, and foods that are composed primarily of each. The circle at the top represents the foods that contain a higher number of micronutrients: vitamins and minerals, which are mainly non-starchy vegetables like leafy greens.
Protein-rich foods include meat and animal products, including fish, eggs and dairy. Fat-rich foods include nuts, seeds and oils like coconut oil, avocado and olives. Carbohydrate-rich foods include starchy vegetables like potatoes, grains, legumes and fruit. Ray concedes, however, that none of these foods are composed of a single macronutrient; animal products often contain a significant amount of fat; nuts and seeds also contain protein and carbohydrates; and legumes and grains contain some protein as well.
Ray points out that most diets, particularly the Standard American Diet, is bottom-heavy. North Americans generally over-consume macronutrient-rich foods that are higher in fats, carbs, proteins, and calories in general, and under-consume micronutrient-rich foods like fruits and vegetables. Because of this, North Americans consistently fail to meet the levels of vitamins, minerals and antioxidants essential for optimal bodily function.
It seems that even “healthy” diets tend to focus on the bottom of the pyramid, restricting certain groups of foods while making up the balance by over-emphasizing others. Paleo and low-carb dieters often fixate on the right side of the pyramid, including animal products, nuts and seeds, but avoiding grains and legumes, while vegan and vegetarian diets concentrate on the left side of the pyramid, eschewing all animal products and getting protein from grains, legumes and nuts instead.
One thing all healthy diets seem to emphasize, however, is fruit and vegetable consumption. When studying the merits of a vegan or paleo diet, it is the non-starchy, micronutrient-rich vegetables that may confer most of the health benefits, regardless of the carb, fat and protein content. Therefore, Ray recommends focusing on the top of his food pyramid, eating as many vegetables as possible, while eating a balance of foods from the base.
Since we rarely eat pyramids, I often depict this balance for my patients using a plate. I divide the plate into four quarters. One half of the plate is dedicated to colourful vegetables, with at least a full quarter dedicated to greens. The other two quarters of the plate are divided into starches: grains, legumes, tuberous vegetables, and proteins: meat, dairy, eggs, fish, or legumes. Oils and fats can be used to cook with or added to the meal in the form of avocados, nuts and seeds.
Listening to the Body as Guide
So, while Ray’s advice to eat as many green and colourful vegetable as we can while eating a balance of the foods at the bottom of the pyramid is sound, how can we establish what the right balance is for us? Many of us will have vastly different requirements for the macronutrients: carbs, fat and protein. My body has an energy demand that is different from that of my 6′ friend who lifts weights daily, or my 90-year old hypertensive, mainly sedentary Italian grandmother. As a naturopathic doctor, who believes in an individualized approach to health, I tend to reject top-down dietary recommendations that ignore the variabilities among people.
A friend of mine, having damaged his health through a string of restrictive dieting, argues that all food—even refined sugar and saturated fat—has a place in a healthy diet. He believes our bodies are designed to crave fat, protein and carbohydrates in ratios that promote optimal health. He writes in his book that we can eat whatever we want as long as we eat intuitively and avoid foods laden with “fake” flavours and processed oils, like corn oil, that confuse our internal cues and hunger signals. He also argues, like the filmmakers in the Netflix documentary, What the Health, that there is no evidence that refined sugar causes diabetes, and that diets based on avoidance of certain foods are detrimental for health.
While I’m not convinced that refined sugar deserves to be completely cleared of all charges, I agree that mindful and intuitive eating may be the key to maintaining balance. Healing with Whole Foods by Paul Pitchford places awareness and physical activity at the base of its Integrative Food Pyramid. The idea is that we need to first establish the foundations of movement and mindfulness before we begin to talk about food intake. As my friend says, perhaps the key is tuning in to our own internal physiological and emotional cues through mindfulness, paying attention to hunger and cravings, rather than measuring calories, carbs, protein, or fat grams.
Following our internal cues may be difficult, as the book TheDorito Affect outlines. The author points out how certain foods are engineered to override our hunger and satiation signals and monopolize our cravings, leading us to overeat. Therefore, if we’re going to follow our body’s signalling, mindfulness is a requirement, but so is following the advice of Michael Pollen, author of The Omnivore’s Dilemma, who famously tells us to “Eat food. Not too much. Mostly Plants.”
Pollen urges us to stick to foods that resemble something we might encounter in nature: eat foods our grandmothers would recognize; purchase foods that come from a plant, not foods that are made in one; and to stick to whole foods or packaged foods with five listed ingredients or less. Pollen also encourages us to cook and prepare as much of our own foods as possible. Do you have a craving for potato chips, ice cream, or dark chocolate? Feel free to indulge, as long as you make it yourself using the raw, natural ingredients. The theory is that, when the body is given clean, whole food, it regulates its hunger and satiety signals to communicate to you exactly what it needs.
Heal the Individual
When it comes to whole foods, I believe that there are no “good” or “bad” foods, generally speaking. Observational studies that examine how traditional societies ate suggest to us that saturated fat, animal protein, dietary cholesterol, and carbohydrates all have a place in a balanced diet. However, when it comes to diet, especially therapeutic diets, it’s my job to consider the individual and their health context: there are no good or bad foods, but some foods are better or worse for certain people, and some may even be better or worse for certain people at certain points along their health journeys.
When I am helping my patients calm inflammation, heal their digestive systems, clear their skin, or manage autoimmune disease, I often recommend identifying food sensitivities and eliminating those foods from the diet. Oftentimes these foods need to removed only temporarily, but sometimes foods may need to be removed indefinitely. Patients with insulin resistance, such as in the cases of obesity, PCOS, diabetes or metabolic syndrome, often do well on a low-carbohydrate diet to restore insulin sensitivity. Again, these anti-inflammatory, reduced-carbohydrate diets may only be required until hormonal balance is restored. Older adults concerned with promoting longevity, or patients undergoing cancer treatment, may do better restricting protein to lower their levels of growth factors, while athletes and stressed out adults may require higher amounts of protein to promote muscle building, or to synthesize mood-regulating neuro-chemicals. A woman who is stressed, depressed, exhausted and iron deficient may feel much better increasing her dietary intake of red meat to help regulate her nervous system. Another woman, with a family history of colon cancer, may do better avoiding it.
Endless factors need to be taken into account when we consider which dietary style is right for us. Our health goals, health status, nutrient status, digestive system health, immune system health, liver functioning, insulin sensitivity and hormone balance, levels of stress, toxic load and inflammation are just some of the things that I consider when making lifestyle recommendations for my patients. Lifestyle preferences, tradition, culture, religious backgrounds, cooking abilities, time constraints, and other factors, will also all play a role in our food choices and eating habits.
Our emotional connection to food and our ethics also matter. While veganism is certainly not a diet I recommend, if consuming animal products is out of line with one’s morals, then following a vegan diet may be the healthiest way for them to live in accordance his or her beliefs. Similarly, someone with a history of disordered eating may need to lift all food limitations, even junk food, in order to heal his or her relationship with food and hunger.
Investigations into the eating patterns of traditional societies tell us that human beings thrive on a variety of different diets. Optimizing diet for the individual goes beyond following the latest research or government and industry-funded health recommendations. It involves eating a variety of natural, whole foods, learning to pay attention to the body’s hunger signals, and even working with a health professional who uses diet to help promote health and manage disease on an individual level.
Sigh… I just finished reading a rather annoying article in the Globe and Mail (don’t even bother to click and add more Google street-cred, seriously) that doesn’t really warrant a response but… here we go. It’s my day off.
The article was written by one Carly Weeks, who doesn’t seem to have a very positive view of naturopathic doctors. I don’t know Carly and have no idea about her health history, but I’m going to take a shot in the dark and imagine she hasn’t suffered from chronic eczema.
Let me know how that steroid cream works out for ya, Carly!
But, ad hominem aside, her issue with naturopathic doctors this week(s)—pun intended, aren’t I hilarious—is, what else: we’re a bunch of quacks who use nothing but false therapies and smooth-talking to coax our patients into thinking they feel better. Well, if that worked, I wonder why more healthcare practitioners don’t try copying those moves too. It might save the government some money, which is what, coincidently, naturopathic medicine is already doing and it’s not by false therapies and smooth-talking. (But we do make time for a lot of talking).
The Globe piece begins with a story about how physicians (not naturopaths, for the record) prescribed radioactive water in the 1920’s. It’s a cute and tragic story about limited safety profiles. And other than its juxtaposition in an article about NDs, I’m not sure what the writer’s point was. We don’t use radioactive water to treat anyone. If you want radiation, which is a therapy, a cancer treatment, then you must see an oncologist. Talk about throwing out babies and bathwater.
The article is largely about how naturopathic doctors are moving under a new regulatory board, under the Regulated Health Practitioners Act. This limits our scope compared to that of provinces like BC or certain US states, where naturopathic doctors have been prescribing drugs and even performing minor surgeries safely where it’s warranted.
Here are some facts:
Naturopathic medicine is incredibly safe. We are trained in conventional diagnosis, anatomy, physiology, physical exams, including gynaecological exams, breast exams and digital rectal exams. We have the ability to perform acupuncture in Ontario and give intramuscular injections. With additional training we can provide IV treatments. We are trained to order and interpret labs and to take blood. I will not deny that conventional medicine and pharmaceuticals have saved millions of lives. However, we know that 10,000 yearly deaths in Canada (and 100,000 in the US) are due to pharmaceuticals alone. A year ago I wrote a post talking about the off-label birth control pill Diane-35. Let’s not start comparing safety profiles here.
Naturopathic doctors are highly trained and educated: We have completed a 4-year very rigorous program that includes a 12-month internship where we treat patients in an out-patient facility. In our training we performed over 100 practical and written examinations. After our second and fourth year we complete two licensing exams, which span a course of 5 full days of examinations combined. Ask anyone I know if what I did was easy. Trick question: they wouldn’t know because they didn’t hear from me for the past 5 years–I was studying the WHOLE time. It’s ok, though, because now I know a lot.
Naturopathic medicine is a regulated profession: In order to practice in Ontario naturopathic medical graduates who have passed both licensing exams, must pass a series of board examinations that are both written and practical. We then must enter into a month-long application process, which includes a police background check and character reference check. If I try to delay treatment of an emergent condition or treat an emergent condition with something like homeopathy or acupuncture (effective treatments for other conditions, but not emergent, life-threatening ones), which is something we are often accused of potentially doing, my licence will be removed. It’s not something we do—it’s that simple. We are held accountable and have a lot of responsibility to deliver safe care.
Naturopathic doctors are health experts: In order to complete the naturopathic medical program we complete 1200 hours of clinical training and 3000 hours of classroom training. This does not include study time for our board exams and pursuit of side interests or continuing education credits that are required to maintain licensure. We are trained in nutrition, which many medical professional, including medical doctors, are not. Naturopathic doctors often see patients that have been failed by the conventional medical system, which means we deal with complex cases on a regular basis. This demands that we keep our skills sharp and our knowledge current.
Naturopathic medicine provides the public with an amazing service that patients are willing to pay for: We spent up to two hours at time with our patients, educating them on any topic of their health picture: the medications they’re on that their doctors don’t have time to discuss with them, their health conditions, their prognosis and what else they can do about it. I spent half an hour talking about an STI a patient of mine had been diagnosed with. She’d seen two doctors and a specialist. None of them had talked to her about it. Patients have told me their doctors no longer perform physicals. Well, we do. And, it turns out, people pay for excellent care. Naturopathic medicine provides the much-needed service of patient education, human-centred care and prevention of disease. It’s an excellent complement to an effective whole-person healthcare strategy.
Naturopathic medicine works: I could say more on this but let’s keep it brief: if it didn’t work, people wouldn’t pay for it. The Globe and Mail, more than anyone should know to “let The Market speak.” (Amiright?) I lied, I will say more. If you don’t think naturopathic medicine works, then call my patients who no longer have chronic pain or allergies or chronic constipation. Ask my patient who couldn’t conceive how her daughter is doing. Blah blah, we help people.
Naturopathic doctors prefer to work in collaboration with other healthcare professionals: Ideally each patient should be managed by a healthcare team. When I start seeing a new patient I immediately establish a relationship with his or her medical doctor. I refer out for labs and to specialists if necessary. Medicine should be integrative, not alternative. Patients shouldn’t be forced to choose.
In addition to accusing us of being a bunch of unsafe quacks, the author writes, “Ontario should have created a regulatory system based on the principle of evidence first.” So, there you have it. Only medicine that is based in evidence should be regulated by the province.
Wow, what a ridiculous statement made by someone who I imagine knows little to nothing about how medicine and so-called “evidence” works.
Firstly, there is more than one type of evidence. In fact, evidence is a hierarchy. At the bottom we have things like clinical case reports or expert opinion, what my friends the skeptics love to call “anecdotal evidence.” Sigh. If you’ve seen something work, you keep doing it. It’s not the best evidence we have, but it’s still evidence. The better forms of evidence, randomized control trials, are being done on naturopathic therapies and naturopathic therapies have been found to hold steady. Actually, many of the therapies we prescribe are done precisely because there is evidence to support it: fish oil for depression and bipolar disorder? Inositol for fertility in patients with PCOS? Evidence, evidence, evidence.
Secondly, only 10% of medical guidelines are based on the type of “evidence” that our friend Carly Weeks is likely referring to: the Randomized Control Trial, which involves comparing two groups: a treatment group to an inactive group that gets something like a placebo. Well, it turns out, we just don’t have that much “evidence” of this sort to dictate what happens in medicine. A tourniquet for a bleeding wound? Using general anesthetic rather than nothing? These things haven’t been compared against placebo. What is the other 90% of medicine based on? Expert opinion: a nice mixture of clinical expertise, intuition, common-sense, “what the heck, might as well try it it couldn’t hurts” and research. I don’t see Carly questioning the use of SSRI for mild and moderate depression or beta-blockers to prevent cardiac events as a result of high blood pressure, both of which have “no evidence” to support their use. Nope, just crickets when it comes to those topics.
Thirdly, the father of EBM, or Evidence Based Medicine, himself, Dave Sackett, said, “Good doctors use both individual clinical expertise and the best available external evidence, and neither alone is enough. Without clinical expertise, practice risks becoming tyrannized by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient.” (Emphasis mine). Individual clinical expertise from both modern and traditional medicine, the best available external evidence and tailoring treatments to individuals patients needs and preferences? Sound like naturopathic medicine to me.
Naturopathic medicine is safe and effective. We have a patient-centred approach and offer wonderful service for the cost, which is often covered by insurance benefits. Naturopathic doctors take the time to listen to your story and educate you on what is happening in your own body. We treat the root cause of your condition, rather than masking symptoms. We are highly-trained healthcare professionals and we are regulated. Soon we will be moving to different regulation. However, the government will be removing some of the rights we’ve had, which include ordering certain lab tests that we’ve safely ordered for years. If you use or support naturopathic medicine, please click the link to sign the petition to maintain the current naturopathic scope of practice in Ontario and support safe and effective natural healthcare for all Ontarians.
My family waste no time making illusions about their lack of acceptance of my form of medicine. If left unchecked, dinner table conversation can quickly lead to arguments about the efficacy of the flu shot, why Cold FX is unnecessary and whether “eating in moderation” includes microwave pizza. Lately I’ve decided it’s not worth the bother to champion my cause; I now simply remain silent, keeping my eyes on my gluten-free toast. Having a family that is not well-versed in natural medicine, however, is educational. It removes me from the naturopathic medicine bubble of my colleagues and ex-classmates and brings me back to reality. The truth is that many people don’t know or can’t appreciate what we naturopathic doctors do. There are several myths I’ve been confronted with, ranging from critically negative to unknowingly innocent, that need to be destroyed.
1. Naturopathic Medicine is not scientific.
The main criticism against naturopathic medicine is that it is unfounded and unscientific. “If alternative medicine worked, it would just be called medicine,” once said Tim Minchin, a comedian that skeptics love to quote. While there are several political reasons for the fact that there are not as many studies on natural therapies as there are on conventional medical therapies, the body of evidence that supports natural therapies is growing. Naturopathic doctors use conventional medicine to diagnose, request laboratory tests and perform physical exams on our patients. We follow many conventional medical guidelines, all of which are evidence-based. In naturopathic medical school, we were taught to consult a wide range of scientific journals for developing our treatment plans. Throughout our education we were required to write research reviews and case studies. The Canadian College of Naturopathic Medicine and its affiliate centres such as the Ottawa Integrated Cancer Centre conduct many research studies and offer research residency programs for graduates of the naturopathic medicine program.
Further, the notion that nutrition is unscientific is ridiculous. We know that what we put in our bodies can either improve or diminish our state of health. Herbal remedies and therapies, such as acupuncture, have been used for millennia. Most drugs are derived from the medicinal properties of herbs.
Additionally, there is an increasing number of medical doctors employing natural therapies in their practices; the reasons being that they are safe, gentle and they work.
2. Naturopathic doctors are anti-pharmaceutical, anti-surgery and anti-vaccine.
The practice of naturopathic medicine involves adhering to the Therapeutic Order. This order is a loose guideline for developing a treatment plan that begins with establishing the conditions for health: a healthy diet, lifestyle and environment, and ends with more invasive therapies not performed by naturopathic doctors, such as powerful medications and surgery. For example, if you break your arm, a medical doctor will set the bones back into place, manage your pain and immobilize the bones by using a cast and sling. However, drugs and surgery do not fuse your bone back together. This magical feat is performed by your body, or what we naturopathic doctors term the healing power of nature. Surgery would not work without it. Our job as naturopathic doctors is to help your body do its job of healing, enabling your bones to heal faster.
Like natural therapies, some conventional therapies are better than others. Some heavy medications are necessary for temporarily managing pain or stabilizing life-threatening acute conditions, such as anaphylactic shock. However, preventing these health crises or working alongside conventional medicine to help the body better recover is the job of the naturopathic doctor.
Naturopathic doctors are not anti-vaccine. Some vaccines are more effective than others and, like many therapies, some vaccines carry with them risks, however small. Naturopathic doctors have medical knowledge and time to spend with patients. We believe in taking the time to share our knowledge and research with patients to help them make informed choices about their health and what goes into their bodies, vaccines included.
3. Patients need to choose between naturopathic and conventional medicine.
There are numerous studies that show that, when practiced together, naturopathic medicine and conventional medicine achieve better outcomes than conventional medicine alone. Naturopathic cancer care, for example, is not about curing cancer with green smoothies; it aims to keep patients feeling healthy and strong while undergoing chemotherapy and radiation so that they can complete their treatment. Many patients with cancer experience negative outcomes because the treatment cannot be completed due to diminishing health or debilitating side effects. For any condition, naturopathic doctors work alongside medical doctors to benefit our patients. The job of the naturopathic doctor is to help strengthen our patients’ health and support their bodies through disease, not compete with medical doctors. Many people term naturopathic medicine Integrative Medicine because it aims to integrate the existing body of medical knowledge, both conventional and natural, to better help patients.
4. You can go to a supplement store; you don’t need a naturopathic doctor.
Natural health products are a complicated issue because, like Advil, they can be acquired without a doctor’s prescription. However, this means that patients become consumers, subject to marketing schemes and misinformation. A naturopathic doctor is a doctor. We take your health history (spending up to 90 minutes doing so) and then spend time developing a comprehensive treatment plan that fits you as an individual. This is far more powerful and effective than simply buying health products on a whim or shooting in the dark. We recommend products at the correct dose and for the appropriate duration. We can also tell you which products have the most evidence behind them. We have studied medicine for 8 years and develop treatment plans, as doctors, to treat your condition. This is vastly different from self-prescribing fish oil because you heard it’s good for you.
5. You should only visit a naturopathic doctor if you’re willing to make drastic lifestyle changes.
There was a time when naturopathic doctors put all of their patients on an extreme diet, such as the Anti-Candida Diet or some facsimile. While many people felt better on this diet – it eliminated many noxious foods such as fast food, processed foods and sugar – it served to intimidate many who didn’t feel ready for such a drastic change. Fortunately for patients, those days are over. While the practice style of the naturopathic doctor can vary, my personal style is to start slowly and not overwhelm. The treatment plan your naturopathic doctor prescribes you will depend on your readiness for change; you will not be pushed into doing anything you are unready for. Naturopathic doctors are also trained in counselling and are able to assess your readiness for change and help motivate you to make health changes at a pace that you feel comfortable with. We are also trained to support you through the process of making changes, ensuring your success and health outcomes.
6. Naturopathic medicine is for the rich.
It is an unfortunate truth that naturopathic visits are not financially accessible for all Canadians. I charge between $95 to $150 for a visit and, even if the visit lasts 90 minutes, this is certainly not cheap. However, the cost of medicine is not cheap, even if it is covered by the government. There is evidence to show that naturopathic medicine saves the individual and the tax payer money; it is far cheaper to prevent disease than treat it. The average patient at my clinic spends $500 a year on naturopathic visits, most or all of which is covered by extended health benefits. In 2014 the Ontario government removed the need to charge HST for naturopathic visits, slightly reducing the cost of naturopathic medicine. Lastly, while supplements and therapies need to be paid for out of pocket, naturopathic doctors tailor their supplement recommendations to your treatment plan and are trained to take your financial situation into consideration when designing a treatment plan.
When we consider all of the things we channel our money towards, I believe that we as a country could afford to dedicate a little more of our salaries to our health. The average Canadian woman spends $1200 a year on cosmetics and personal care products. However, real beauty comes from being healthy—cultivating a healthy glow from the inside out. Health is your greatest asset; perhaps we should invest in it if we have the means. For those who simply cannot afford naturopathic medicine there are free satellite clinics staffed by interns and cost-effective options such as community acupuncture that provide natural medicine at a more affordable price.
7. Naturopathic medicine is for granola-munching hippies.
Even though my website and business cards are covered in flowers (flowers are beautiful!), naturopathic medicine aims to include everyone, no matter what their value system is. Naturopathic medicine is for people who value their health. It is for those who believe that healing is more than suppressing symptoms and remaining medicated for the rest of their lives. Naturopathic medicine offers an option to anyone who wonders how their lifestyle and diet may be affecting their health. We believe in empowering people to lead healthier lives and to take a more active role in how they feel mentally and physically. We use science, clinical experience and traditional therapies to help people feel better. You don’t need to be a vegan to appreciate what good health is worth.
What other natural health myths have you heard that require destroying?
It seems that, for every person who embraces the idea of holistic medicine with open arms and an open mind, there is at least one skeptic who refuses to acknowledge that alternative medical practices not only exist, but are growing in popularity, helping thousands of people and, most likely, are here to stay.