We’ve been hearing quite a lot about The Science these days. So, what is science? How does science guide medical practice and naturopathic medicine?
The science council defines science as, “the pursuit and application of knowledge and understanding of the natural and social world following a systematic methodology based on evidence.” The answer is, science is a methodology.
It is applied in medicine through Evidence Based Medicine (EBM) which starts with the individual patient and incorporates: clinical expertise, scientific evidence (that best that exists according to a hierarchy), and patient values and preferences.
“Evidence medicine is the conscientious, explicit, judicious and reasonable use of modern, best evidence in making decisions about the care of individual patients. EBM integrates clinical experience and patient values with the best available research information.”
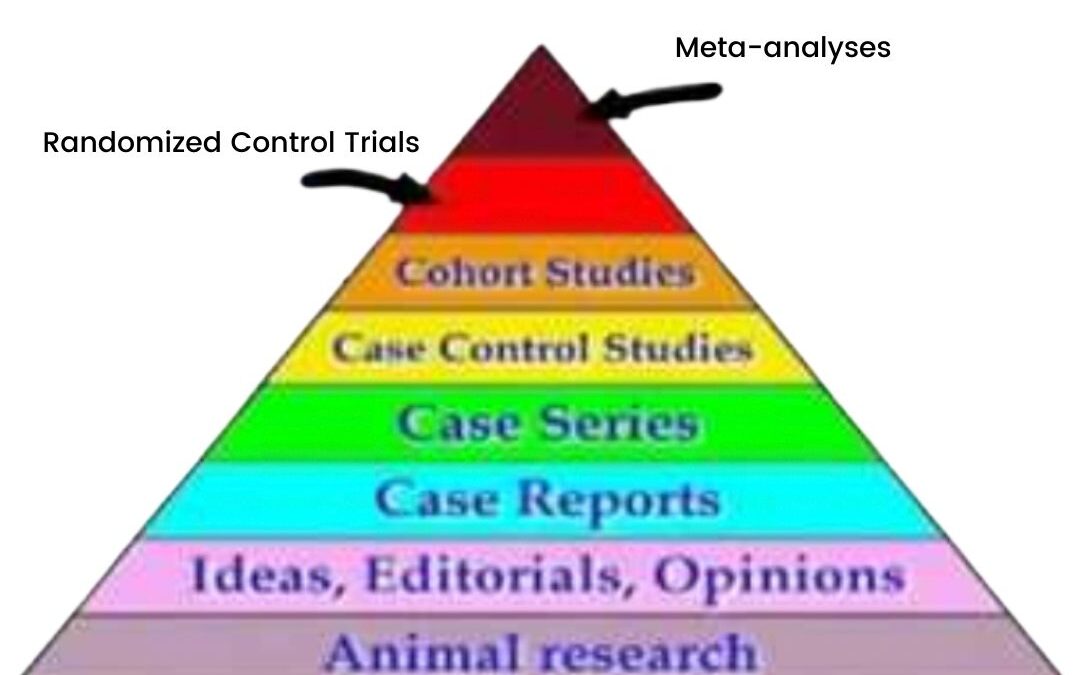
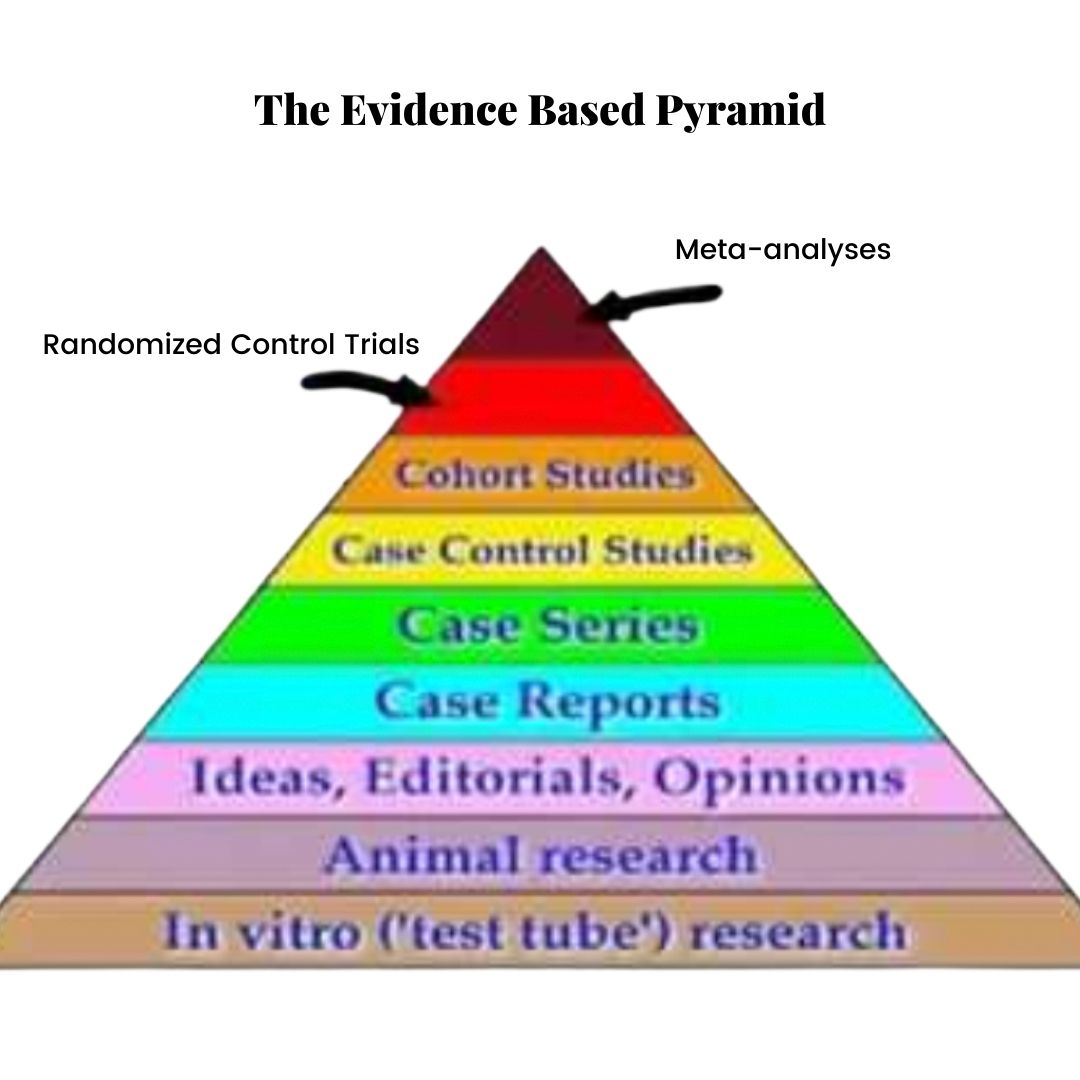
The Evidence-Based Pyramid
In EBM, evidence exists in a hierarchy, represented by the Evidence Based Pyramid (shown above). Animal studies are at the bottom, case reports (clinical anecdotes) somewhere in the middle and randomized control trials and meta-analyses (the Gold Standard of evidence) at the top.
Dave Sackett (the Father of EBM) et al. write in the British Medical Journal (1996),
“Good doctors use both individual clinical expertise and the best available external evidence and neither alone is enough.”
In addiction to scientific evidence, EBM must incorporate:
Patient values
A bottom-up approach (it is patient-centred, not guideline-centred)
The needs of the individual (EBM is not a one-size-fits-all formula)
Clinical expertise
The best available evidence: this does not mean using only randomized control trials. Sometimes the best evidence we have are case reports, historical and traditional use of an herb or animal studies. We still owe our patients the opportunity to see if a treatment works for them, especially if the risk of a given treatment is low.
As clinicians, we use our knowledge in different ways. We start with an assessment of the individual in front of us. This assessment takes into account the factors that influence this patient’s life, their lifestyle, their health condition and their overall health goals.
We then turn to clinical experience, research, our scientific knowledge and guidelines.
We share this information with our patient. Our job is to educate and convey the options so that the individual can provide informed consent. How does this knowledge fit into the patient’s life? How does it inform their choice?
Science is not a set of values. It is not a religion. We do not follow it.
Science provides us with a methodology for seeking the answers to questions we might ask about how the principles of nature, including the human body, are organized.
Science encourages us to ask questions and testing hypotheses in order to find answers.
It is never settled.
Most of all, science doesn’t tell us how to use scientific knowledge.
Our choices are governed by our goals, preferences and values.
So, “follow the sicence?”
No. Follow your goals, preferences, values and dreams.
And use science to help guide your way.
Reference:
Sackett, D. L., Rosenberg, W. C., Gray, J. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. BMJ, 312(7023), 71–72.
In September of 2019, Jakobsen, Gluud and Kirsch published a review in the British Medical Journal: Evidence-Based Medicine entitled “Should antidepressants be used for major depressive disorder?” (1)
Their conclusion was this:
“Antidepressants should not be used for adults with major depressive disorder before valid evidence has shown that the potential beneficial effects outweigh the harmful effects.”
Now, before we move on with what drove them to make this seemingly radical conclusion, I want to be clear:
I am not stigmatizing medication.
All of those who take medication for depression have asked for help.
Asking for help is important.
Asking for help is brave.
And, whatever help works for you is the right kind of help.
But imagine this; imagine you are a pretty decent swimmer.
You’ve practiced swimming all your life. You’ve gotten lots of experience swimming in pools, lakes, and oceans. You know how to swim, just like you know how to cope with turmoil. But, despite your strength, one day you find yourself drowning.
“No, I’m not drowning,” you might say at first. “I can’t be drowning. I know how to swim! If I’m drowning, it means I’m a failure…
“What will everyone think?”
And so you continue to splash around a bit, until it becomes undeniable. You gasp some water-filled air. Your head submerges and you think, indeed, “I’m drowning.”
When you get your head above water you call for help.
This takes a lot.
It’s not easy to admit that you need help.
It’s not easy to overcome that little voice that tells you that asking for help is troubling other people, admitting defeat, showing weakness—and whatever else that darned little voice thinks it means.
“HELP!” You exclaim, louder this time—little voice be damned.
“HEEELP!”
And someone on shore sees you. They have a life-preserver in their hands and they throw it your way.
Your shame is peppered with relief—and gratitude: there’s an answer to all this suffering. You thrust your hand towards the life preserver, grasping it with a firm bravery.
Only, it starts to sink. It’s full of holes.
“What’s the matter?” The person waiting on the shore exclaims, as you continue to struggle, “Don’t you want help?”
The shame returns. Hopelessness joins it.
I advocate for mental health awareness. I advocate for perpetuating the message that it’s ok to talk about mental illness. It ok to admit you need help.
I believe the following:
Depression is not a a sign of weakness.
It’s not a sign that you are defective.
It’s not a sign that you haven’t learned proper coping skills, or that your coping skills are defective, or that you’re fragile.
It’s also not fixed by simple solutions like eating salad, running or putting “mind over matter”.
Depression happens to a lot of us.
It affects 300 million people globally. It is the leading cause of disability world-wide, with a lifetime prevalence of 10 to 20%. This means that 1 in 5 people will experience depression in their lifetimes.
We all know someone who suffers. Maybe you suffer.
And a lot of people ask for help. The National Health and Nutrition Examine Survey (NHANES) in 2017 found that 1 in 8 people over the age of 12 are taking an anti-depressant, a 65% increase over the last 15 years.
This means that 65% more of us are asking for help.
That’s a lot of life preservers.
So, just how effective is this help?
First, we need to understand how the efficacy of anti-depressants are measured.
The symptoms of depression are subjective. This means they are not observable. There is no imaging that shows if someone is depressed. There are no blood tests for depression. There are no physical exams.
Therefore, to assess the presence and severity of depression, clinicians use questionnaires. The most commonly used depression questionnaire is The Hamilton Depression and Rating Scale (HDRS), a 52-point checklist that assesses various symptoms of depression and rates them on a scale of no-depression to severe.
When patients with depression first see a family doctor or psychiatrist they are often issued the HDRS and given a score.
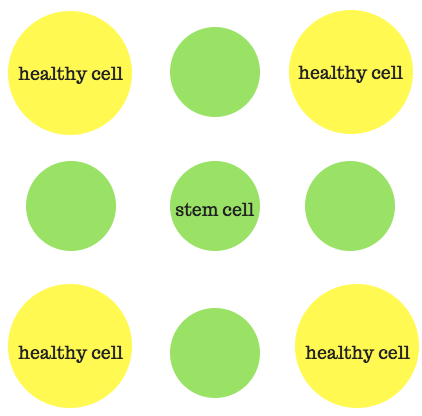
Let’s use Janet’s story as an example. Janet first came to see her psychiatrist two years ago. She wasn’t sleeping and yet felt sleepy all the time. She’d gained weight but had no appetite. Her entire body was sore, as if she had the flu. She’d lost interest in all of the activities that used to fire her up. She’d lost interest in everything.
After a few weeks of feeling progressively worse, Janet began to be plagued by thoughts of suicide. This scared her. She went to her family doctor, who referred her to a psychiatrist.
Janet’s HDRS score was 25. This meant she was moderately to severely depressed.
Janet was given an anti-depressant, a Selective Serotonin Re-uptake Inhibitor (SSRI). She was told it would correct her “brain imbalance”, and treat the cause of her symptoms. Janet was relieved that there was a solution.
If an anti-depressant can decrease the HDRS by 3 points, then the medication “works”. Or at least the results are statistically significant.
However, if Janet’s symptoms improve by 3 points, from a score of 25 to, say, a score of 22, how does she feel?
Not much different, it turns out.
To experience “minimal improvement”, a decrease in symptoms that someone with depression would notice, say an increase in energy, an improvement in sleep, or a change in mood, a patient’s HDRS score would need to decrease by at least 7 points.
This means the Janet would need to bring her HDRS down to 18 or lower before she starts to feel noticeably better.
Studies show that anti-depressants, on average, don’t do this.
Some randomized control trials do show that anti-depressants decrease the HDRS score by at least 3 points, which is still registered by patients as having no perceptible effect, but the results are mixed.
A large 2017 systematic review showed that anti-depressants only decreased patients’ HDRS by about 1.94 points (2) and another large study published in the Lancet (3) also failed to show that anti-depressants produce a statistically significant effect, let alone a clinically significant one.
In addition to the minimal changes in symptoms, anti-depressant research is also polluted with for-profit bias. Most studies are conducted or funded by the drug companies.
This makes a difference: an analysis showed a study was 22 times less likely to make negative statements about a drug if the scientists worked for the company that manufactured it (4).
Studies at high-risk of for-profit bias were also more likely to show positive effects of a drug (5).
Another limitation of anti-depressant trials is the lack of active placebo control. In Randomized Control Trials, participants are sorted into two groups: an active group, in which they receive the medication, and a placebo group, in which they receive an inert pill.
The goal of this process is to control for something called the “meaning response”, or “placebo effect” where our expectations and beliefs about a therapy have the potential to affect our response to it.
Remember that depression, as I mentioned before, is a condition made up of subjective symptoms.
If I asked you to rate your energy on a scale of 1 to 10, how would you rate it? What if I asked you tomorrow? What if I asked you after giving you a drink of something that tastes suspiciously like coffee?
Because of its subjective nature, and the subjective questionnaires, like the HDRS, that measure it, depression is very susceptible to the placebo response.
Therefore, it’s important to control for the placebo response in every trial assessing anti-depressants.
But it might not be enough to just take a sugar pill that looks like an anti-depressant.
SSRI medication produces obvious side effects: gastrointestinal issues, headaches, changes in energy, and sleep disturbances, to name a few.
When a patient taking a pill (either placebo or active treatment) starts to feel these side effects, they immediately know which group they have been randomized to, and they are no longer blinded.
This can be solved by giving an “active placebo”: a placebo that produces similar side effects to the active medication. Unfortunately anti-depressant trials that use active placebo are lacking.
But what about the people who DO benefit from anti-depressants?
Janet knew a few. She had a cousin who also suffered from depression. He took medication to manage his symptoms. He’d told her many times that he just wasn’t the same without it.
Perhaps you, reading this article have found benefit from an anti-depressant medication. Perhaps you know someone who has: a family member, or a friend. Maybe it was their lifeline. Maybe it’s yours.
According to Jakobson et al., there are indeed some people who benefit from anti-depressants. Anecdotally we know this to be true. However, the results of large studies show minimal to no benefit from medication, on average.
This means that some people might benefit; we know that some do. It also means that an equal number of people are harmed.
In order for the net effect of anti-depressant medication to be close to zero, an equal number of people experience negative effects that outweigh the positive effects seen in others.
So, while some may have already tried medication and benefited from it, those considering medication won’t know if they’ll be in the group who benefits, or the group who is harmed.
The side effects of anti-depressant medication are often underrepresented. In the Lancet study, adverse effects were neither recorded nor assessed (3).
The most common side effects include gastrointestinal problems, sleep disturbances, and sexual dysfunction. More serious side effects, like increased risk of suicide, are also possible. Some of these effects may persist even after the medication is stopped.
Anti-depressant trials are short-term. Most trials assess patients for 4 to 8 weeks, while most people take anti-depressants for 2 years or longer.
Anti-depressants also put people at risk of physiological dependence and withdrawal.
Withdrawal symptoms can occur a few days, or even weeks, after tapering anti-depressant medication. They sometimes last months.
Withdrawal symptoms are often mistaken for depressive relapse. This can make it difficult, or even impossible, for patients to come off medication. This is worrisome considering the lack of research on long-term medication use.
It is sometimes argued that anti-depressants are more effective, or even essential, for severe depression, however the evidence for this is lacking (4).
In their paper, Jakobson, Gluud and Kirsch conclude that, based on the evidence, anti-depressants show a high risk of harm with minimal benefit.
Before prescribing them, Jakobson et al recommend more non-biased, long-term studies that use active placebo, and honestly assess the negative effects of the medications.
They recommend that studies use improved quality of life and clinically meaningful symptom reduction, not just statistical significance, as standards for treatment success.
Despite these conclusions, SSRIs remain a first-line treatment for major depressive disorder. They are also prescribed for conditions like severe PMS, IBS, anxiety, grief, and fibromyalgia, or other pain conditions. 1 in 8 adults in North America are taking them.
As a clinician who focuses in mental health, I am not against medication.
I have seen patients benefit from SSRI or SNRI medications. Sometimes finding relief with medication when nothing else worked.
My clinical practice keeps me humble.
If a patient comes into my practice on medication, or considering medication, I listen. I ask how I can support them. I answer questions to the best of my ability. I trust my patients.
Patient experience trumps clinical papers.
However, for every patient who benefits from medication, just as many experience negative side effects, or no effect. I trust their experiences too.
I also trust the experiences of the patients who have been trying for months, or years, to wean off medications.
Let me repeat it again: depression is real. Asking for help is hard. And it’s important.
Depression is a multi-factorial condition.
This means that it stems from hundreds of complex causes. This is why it’s so difficult to treat. This is why so many people suffer.
Let me also repeat: depression is not easily fixed.
There is no one solution, and there are certainly no ONE-SIZE-FITS-ALL solutions.
So, if you or someone you care about is suffering from depression, what can you do?
First, get help. This is not something you can get through alone.
Second, seek lots of help: gather together a team of professionals, family and friends. You can start with one person: your family doctor or a naturopathic doctor, and then assemble your support network.
Choose people you trust: people who listen, provide you with options, and seek your full informed consent.
It is important to work with a healthcare team who take into account the factors that may be contributing to your symptoms: brain health, gut health, life stressors, nutrition, inflammation levels, presence of other health conditions, sleep hygiene, family history, contributing life circumstances, such as grief, trauma, or poverty, and who lay out various treatment options while filling you in on the risks, benefits and alternate therapies of each.
Medication may be part of this comprehensive treatment plan, or it may not.
It is brave to ask for help.
And I believe that bravery should be rewarded with the best standard of care—with the best help.
References:
Jakobsen JC, Gluud C, Kirsch IShould antidepressants be used for major depressive disorder?BMJ Evidence-Based Medicine Published Online First: 25 September 2019. doi: 10.1136/bmjebm-2019-111238
Jakobsen JC, Katakam KK, Schou A, et al. Selective serotonin reuptake inhibitors versus placebo in patients with major depressive disorder. A systematic review with meta-analysis and trial sequential analysis. BMC Psychiatr2017;17:58
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. The Lancet2018;391:1357–66
Kirsch I, Deacon BJ, Huedo-Medina TB, et al. Initial severity and antidepressant benefits: a meta-analysis of data submitted to the food and drug administration. PLoS Med2008;5:e45.doi:10.1371/journal.pmed.0050045
Ebrahim S, Bance S, Athale A, et al. Meta-Analyses with industry involvement are massively published and report no caveats for antidepressants. J Clin Epidemiol2016;70:155–63.doi:10.1016/j.jclinepi.2015.08.021
My friend Nelson (not his real name) was depressed.
Depression frequently came in and out of Nelson’s life, but this last bout was the worst.
Severe job stress compounded by issues with his relationship sent Nelson into a downward spiral, leaving him broken, sobbing and exhausted after engaging in the simplest of tasks.
Sadness and a feeling of doom rushed in to greet him at the end of each sleepless night. Nelson gained weight, despite never truly feeling hungry. His face appeared sunken and swollen. Despite sleeping 14 hours a day, dark circles hung under his eyes.
Since focusing and concentrating on work was impossible, he asked his psychiatrist to help him apply for mental health leave. Nelson was granted sick leave, as well as a prescription for Effexor, and a recommendation to get as much rest as possible.
After a year, Nelson felt worse. When rest and the medication weren’t working, he started exercising vigorously. He hired a nutritionist who cleaned up his diet, and he started taking fish oil and a B complex, among other supplements.
Even then, he still struggled. The hopelessness was still there. Returning to work at this point seemed impossible.
Nelson opened up to a friend about his struggles.
“I went through a similar thing a few years ago,” Nelson’s friend confessed. “And the thing that helped the most was micro-dosing.”
Micro-dosing, taking small doses of psychedelic substances, like LSD or psilocybin-containing “magic” mushrooms, entered the public consciousness in early 2015, after James Fadiman, PhD and author of The Psychedelic Explorer’s Guide, appeared on the Tim Ferris Podcast.
It involves taking a “sub-perceptual” dose of a hallucinogen, like LSD or Psilocybe cubensis “magic” mushrooms, that contain the hallucinogen psilocybin. A sub-perceptual dose means that, while these substances still exert effects, they don’t produce a noticeable hallucinogenic “high”.
According to Paul Austin at the The Third Wave, people micro-dose for two main reasons: to remove negative mood states, such as depression, anxiety, PTSD, addiction, and ADD; and to increase positive mood states such as flow, creativity, improved productivity and focus, and sociability.
Micro-dosing has been used experimentally in individuals trying to quit smoking and to heal depression.
After listening to the podcast and reading some of the articles his friend sent him, Nelson managed to obtain capsules containing 200 mg of dried psilocybin mushrooms. Procuring these substances is still illegal, but Nelson figured he had nothing to lose.
When I caught up with Nelson, he was already a few weeks into his micro-dosing regimen. I asked him how he was doing.
“I’m actually feeling better than I have in months,” he told me, smiling. “I’m not passing out on the couch anymore. I wake up at 7 every morning without an alarm. I feel optimistic for the first time in months. And it seems to be consistent!
“This week I’ve managed to attend three social events and I seem… more motivated. My workout game improved too. Also, I’m not sure I’m ready to go back to work just yet but I’ve noticed my motivation has picked up. So much so that I’ve started taking free programming courses online. I—I can’t really believe it.”
Research on Psychedelics for Depression
Unfortunately, we can’t draw any sound conclusions from Nelson’s experience; scientific data from randomized control studies is still lacking. However, the growing collection of anecdotes on the benefits of micro-dosing for mental health and well-being has caught the attention of researchers.
Thomas Anderson, a PhD candidate at the University of Toronto, polled almost one thousand participants on social media channels and message boards, like Reddit, to gather some initial data on the benefits and drawbacks of micro-dosing hallucinogens.
The micro-dosers that Anderson and his team polled reported higher levels of creativity, and improved mood and focus. They claimed to notice a reduction in depression and anxiety symptoms, increased motivation to eat right and exercise, cognitive enhancement, improved self-efficacy and heightened social functioning.
They reported that the main drawback they experienced was obtaining these substances, which are currently illegal in The US and Canada.
Although interesting, this self-reported data isn’t hard science. To increase objectivity, Anderson and his team presented the participants with tests of creativity (finding out how many uses they could find for common objects, for instance) and questionnaires that measured wisdom. The micro-dosers scored high on both these metrics. They also scored lower in tests that measured negative emotion.
Anderson and his colleagues plan to publish these preliminary findings in a series of papers. They are currently in the process of obtaining Health Canada approval for a controlled study.
Psychedelic research was terminated in the 1960’s, leaving a massive knowledge gap of their therapeutic potential. But now, with the publication of Fadiman’s Psychedelic Explorer’s Guide and Michael Pollen’s even more recent How to Change Your Mind, psychedelics are receiving a fresh surge of interest, particularly for their mental health benefits.
One of the prominent names in this new-wave research community is Robin Carhart-Harris, PhD, at Imperial College London, who is investigating psilocybin as a treatment for severe depression.
Published in a 2016 issue of Lancet Psychiatry, Carhart-Harris administered two doses (one small and one moderate) of psilocybin, spaced one week apart, to twelve patients with Major Depressive Disorder. The doses were administered in a controlled, therapeutic setting, and symptoms were rated immediately after therapy, and then again at one and three months.
The study results were remarkable. Five of the twelve patients dropped from “severe depression” to “no depression” immediately after receiving the second dose. All of the study participants experienced an overall reduction in symptoms with five of the study participants remaining depression-free after three months.
Roland Griffiths, Phd, at John Hopkins, is involved in a number of studies examining psilocybin’s ability to induce mystical experiences in terminally ill patients.
In a 2016 randomized, double-blind, placebo-controlled crossover trial published in the Journal of Psychopharmacology, he and his team found that administering high-dose psilocybin to terminally ill cancer patients increased mood, quality of life and optimism, and decreased death anxiety. These benefits were sustained at the six month follow-up. Over 80% of the study participants claimed to experience greater life satisfaction and feelings of well-being.
How Psychedelics Work to Boost Mood
LSD, psilocybin, and other psychedelics, work like serotonin in the brain by acting on serotonin receptors, specifically the 5HT2A serotonin receptors.
Like psychedelics, anti-depressant medications, like SSRI and SNRI medications (Selective Serotonin and Selective Serotonin and Norepinephrine Re-uptake Inhibitors), Cipralex and Effexor, respectively, also work on serotonin pathways. However, these medications’ effects are limited: some people improve on them, while others feel no different, or even worse.
SSRI and SNRI medications activate 5HT1A receptors. According to Carhart-Harris, this makes a difference. In his paper on the “Bipartite Model of Serotonin Signalling” he proposes that these receptor pathways help people cope differently.
5HT1A receptors, acted on by anti-depressants, help with “Passive Coping”. They help individuals with depression tolerate the stress in their lives, be it a toxic work environment or destructive relationship—nothing has changed about the situation, you can just deal with it better.
Psychedelic stimulation of 5HT2A receptors activate pathways involved in “Active Coping”: identifying and directly addressing sources of stress. Active coping might mean asserting boundaries at work or applying to new jobs. It might look like ending an unhealthy relationship.
In other words, 5HT2A receptors stimulate neural pathways that reveal previously elusive solutions to problems. They do this by increasing a chemical called Brain-Derived Neurotropic Factor, or BDNF.
BDNF promotes the growth of new brain cells and neural pathways in the brain. These processes, called “neurogenesis” and “neuroplasticity” , are essential for learning, creativity and memory. Research shows that increased neuronal plasticity benefits mood.
Psychedelics also work by disconnecting the brain’s Default Mode Network. The Default Mode Network, or DMN, connects frontal areas of the brain, such as the Medial Prefrontal Cortex, with lower brain areas like the Posterior Cingulate Cortex.
When we’re daydreaming, stuck in traffic, sitting in a waiting room, or otherwise not actively engaged in a mental task, our DMN lights up. In these quiet moments, we lapse into a state of reflection and self-referential thinking. In other words, our minds wander.
If we’re in a good mood, this mind-wandering creates narratives, daydreams and fantasies about the future. If we’re depressed, it leads to rumination, negative over-thinking, and self-criticism, which worsens mood.
Disrupting the DMN allows old thought patterns to fall away, opening up novel possibilities.
Activating Flow States
Shutting off the DMN can help us enter a state of Flow. Flow states occur when we are completely immersed in an activity so worthwhile that our sense of time and self cease. When in flow, we toe the limits of our talents, making these states incredibly rewarding and enriching. They are the antithesis to depressive and anxious mood states.
Psychedelic substances, along with other practices like meditation, help put us in a state of flow. These states are characterized by elevated levels of serotonin and dopamine and calming and focussing alpha brain wave oscillations. When in them, we become capable of incredible things.
In The Psychedelic Explorer’s Guide, James Fadiman writes about “Clifford”, a premed student. Clifford shares,
“I was taking a biology course to prepare for medical school, and we were studying the development of the chick embryo…I realized that in order to stay alert, a tiny dose of LSD could be useful.
“With that in mind, I licked a small, but very potent, tablet emblazoned with the peace sign before every class. This produced a barely noticeable brightening of colours and created a generalized fascination with the course and my professor, who was otherwise uninteresting to me.”
Due to some health issues, Clifford ends up missing the final exam. His professor agrees to a make-up. Before the exam, Clifford pops the rest of the now-tiny LSD tablet into his mouth.
The make-up exam consists of drawing the complete development of the chick from fertilization to hatching—the entire course.
“As I sat there despondently, I closed my eyes and was flooded with grief. Then I noticed that my inner visual field was undulating like a blanket that was being shaken at one end. I began to see a movie of fertilization!
“To my utter amazement, I was able to carefully and completely replicate the content of the entire course, drawing after drawing, like the frames of animation that I was seeing as a completed film!
“It took me an hour and a quarter drawing as fast as I could to reproduce the twenty-one-day miracle of chick formation. Clearly impressed, my now suddenly lovely professor smiled and said, ‘Well, I suppose you deserve an A!’ …the gentle wonder of life was everywhere.”
While impressive, Clifford’s account, like Nelson’s, is merely an anecdote. Far more research is warranted.
Micro-Dosing for Mood
Micro-dosing allows individuals to tap into the 5HT2A receptor-stimulating, BDNF-increasing, DMN-uncoupling, and flow state activating benefits of psychedelics, without the mind-stabilizing effects.
At a sub-perceptual doses there are no weird colours and visuals, alternate realities, or ego deaths. Micro-dosers report that the world merely appears brighter, or that they feel “sparklier”—they experience greater well-being. Otherwise, they can proceed with their lives normally.
Fadiman’s micro-dosing protocol consists of taking a tenth of a full dose, about 10 to 20 mcg of LSD, or 200 to 500 mg of dried-weight psilocybin mushrooms, every three days. This means that if the first dose is taken on Monday (Day 1), then the second dose is taken on Thursday (Day 4). According to Fadiman, spacing doses avoids tolerance, keeping the doses effective.
Participants are encouraged to engage in their daily activities: working, eating, sleeping and exercising normally.
Fadiman recommends participants keep a record of mood, cognition, motivation and productivity. People often report that they feel the best on Day 2, the day after taking a micro-dose.
Drawbacks to Micro-Dosing
In my role as a naturopathic doctor, I can’t recommend or counsel on the use of psychedelic substances for the treatment of any health condition. While the scientific interest in their use as therapeutic agents is growing, these substances are illegal to obtain and possess, and there is a lack of solid research on their safety and efficacy.
As of right now, the only way to legally access psychedelic therapies is through research. MAPS, the Multidisciplinary Association for Psychedelic Studies, often lists recruitment opportunities for ongoing studies. Thomas Anderson, at the University of Toronto, is in the stages of obtaining Health Canada approval for a randomized control trial on the benefits of micro-dosing in healthy volunteers.
Like all therapies, there are risks to taking these substances, even at low doses. While LSD and psilocybin confer a low risk for addiction and are ten times less harmful than alcohol (the harm scores of LSD and psilocybin are 7 and 5, respectively, compared to 72 for alcohol), they are not completely benign.
Psychedelics can aggravate schizophrenia, psychosis, dissociation, severe anxiety, and panic. They can also interact with medications and supplements that act on serotonin pathways. Their effects at high doses can be disorienting and oftentimes unpleasant: in the studies that showed positive benefit, they were administered under careful supervision, in a therapeutic set and setting.
Our society’s mental health is in crisis. As a clinician who focuses on mental health, I am always excited to learn of new therapies that have the potential to heal mood. With Canada’s 2018 legalization of cannabis, gateways are opening for future uses of psychedelics as medicine. Perhaps with more research and advocacy, we’ll one day see micro-dosing of psychedelic substances as a safe and effective mainstay therapy for promoting mental and emotional well-being.
I will die in here today, I thought to myself, as I sat hunched and cramped in an oven-hot temazcal, or sweat lodge, somewhere on the Mexican pacific.
The straw flap covering the opening of our sweaty mud hut was thrown off momentarily by someone outside, flooding our hellish cave with light. I gazed hopefully at the entrance: were we getting water? Were they letting in fresh air? Was it finally over?
It was none of those things. Instead of relief, they were increasing the heat; a pile of hot rocks appeared at the door.
“Gracias, Abuelita“, said our leader, Marciano, receiving a giant steaming rock with metal tongs and pulling it inside the hut. The change in temperature was immediate. The heat coming off the rocks was like fire. I struggled to breathe.
Marciano is Spanish for martian, abuelita an affectionate term for “grandmother”. Did he know what he was doing, this martian? Was there even enough oxygen in here for all of us? I am not related to these rocks, I thought.
“Gracias, Abuelita,” We numbly replied, thanking the rocks and fanning ourselves with imaginary cool air.
The hut was crowded with ten people. I had to sit hunched over and there was no space to lie down. If I wanted to leave, everyone else would have to get out first. The combination of darkness, stifling humidity, claustrophobic quarters and angry heat was almost intolerable. Sweat was pouring so profusely off my body that I had become one with it.
Every cell of my body was on fire with craving: water, space to lie down, fresh oxygen, freedom.
Whenever I thought I couldn’t stand another moment, the heat intensified.
The tiny flap in the door opened again. Another grandmother rock from Mars? No, it was water! My heart flooded with gratitude until I realized that the tiny glass being passed around was for all of us to share.
I will die in here.
I will never again complain of ice and snow.
This is supposed to be therapeutic?
When it was over, I emerged gasping desperately for air and water. After chugging a bucketful of water, I dumped another on my scorching hot skin. I swear it emitted a hiss.
I had survived! However, as my body cooled, I realized that I had done more than survive. Despite my resistance throughout its entirety, the sweat lodge had left me feeling absolutely elevated.
The feelings of energized calm lasted well into the next few days. My brain seemed to work better, evidenced by an elevation in the fluency of my Spanish.
It was amazing.
Current research shows that heat therapy, like sweat lodges and saunas, can indeed be therapeutic. Subjecting the body to high temperatures can improve the symptoms of major depressive disorder as effectively as the leading conventional therapies, such as medication.
Intrigued by the cultural practices of using intense heat to induce transcendental spiritual experiences (the Native American sweat lodges and Central American temazcales, for instance), a psychiatrist name Dr. Charles Raison decided to investigate heat as a therapy for improving mental and emotional well-being.
Raison and his team, in their 2016 JAMA Psychiatry study, took 60 randomized individuals suffering from major depressive disorder, and subjected them to a standardized questionnaire, the Hamilton Depression Rating Scale (HDRS), which quantifies depressive symptoms. The treatment group received Whole Body Hyperthermia, an average of 107 minutes in an infrared heating chamber that heats core body temperatures to 38.5 degrees celsius.
The placebo group spent the same amount of time in an unheated box that was nearly identical (complete with red lights and whirring fans). 71.5% of the study participants who were put in the sham heating chamber believed that they were receiving the full heat therapy.
After one week of receiving the single session of heat therapy, the active group experienced a 6 point drop on the HDRS. This decrease outperformed even the standard anti-depressant treatment, selective serotonin re-uptake inhibitor medications (according to a 2017 meta-analysis SSRI medications drop patients only 2 points on the HDRS), and lasted for 6 weeks.
Previous fMRI research has shown that heat sensing pathways in the skin can activate brain areas associated with elevated mood, such as the anterior cingulate cortex (the ACC is also activated during mindfulness meditation). The raphe nucleus, which releases serotonin, our “happy hormone”, is also activated by this skin-to-brain thermoregulatory pathway.
Heat is also thought to calm immune system activation present in the brains of individuals suffering from depression. People with depression tend to have higher body temperatures than non-depressed people. This is possibly due to the present of inflammatory cytokines, such as TNF-a and IL-6, that increase inflammation and fever and have been shown to negatively impact mood. Perhaps heat therapy acts by “resetting” the immune system.
Furthermore, when the body is exposed to high temperatures, it results in the release of heat shock proteins. Heat shock proteins respond to short, intense stressors: hot, cold, and even fasting conditions. They have a variety of effects on our hormonal systems. Some can reset the body’s stress response, correcting the cortisol resistance that is present in the brains of depressed individuals. One particular heat shock protein, HSP105, has been shown to prevent depression and increase neurogenesis (the creation of new brain cells) in mice.
Reduced neurogenesis in the hippocampus is a risk factor and side effect of depression. It is thought that traditional anti-depressants, in addition to altering brain levels of serotonin, may exert some of their effects through inducing brain-derived neurotrophic factor (BNDF), a growth factor that encourages the development of new brain cells.
Conventional theories tell us that depression is a disorder resulting from a chemical imbalance in the brain requiring medication to “correct” that imbalance. However, an overwhelming amount of research tells us that this is simply incorrect: depression is a complicated condition stemming from multiple causes.
Naturopathic doctors focus on the whole person. We look at how an individual’s symptoms are expressed within the context of their biology, physiology, psychology, and social and physical environments. We know that, when it comes to a condition like depression, every body system is affected. We also know that the health of our digestive and hormonal systems are essential for optimal mood.
Naturopathic doctors have also traditionally used hydrotherapy, the therapeutic application of hot and cold water, to benefit digestion, boost detoxification pathways, and regulate the immune system.
Therefore, as a naturopathic doctor, the idea that heat exposure can have a profound effect on depressive symptoms makes sense. However, as a clinician, I’ve found it difficult to convince my patients suffering from depression to try heat therapy. Perhaps it’s because the remedy seems so simple it borders on insulting—sweat for an hour and experience profound changes to a condition that has debilitated me for months? Get out of here.
I get it.
However, research suggests that since depression is a multi-factorial condition, it deserves to be addressed with a variety of therapies: diet, sleep hygiene, exercise, nutrition, and psychotherapy, to name a few. Heat therapy can be another important one.
So, here are some suggestions for implementing heat therapy without having to do a sweat lodge:
If you have access to a sauna, us it! Alternate 15 to 20 minute stints that induce sweating with 60-second cold rinses in a shower. Cycle back and forth for up to an hour.
Go to a hot yoga class a few times a month.
Exercise. Exercise has been shown to induce temperature changes that are similar to heat therapy. This may be why exercise has been so well studied for its mental health benefits.
Take epsom salt baths regularly. Add 1 to 2 cups of epsom salts to a warm bath and soak for 20 minutes or more, or to the point of sweating.
Try Alternate Hot and Cold Showers: alternate between one-minute bursts of hot water and 30-seconds of cold for about 3 to 5 cycles.
In the past I used to suffer from “hanger”, feeling hungry and irritable if going more than a few hours without food. Now my body is adapted to fasting, going prolonged periods without food—and I feel all-the better for it.
When I was a kid, no one ever had to convince me to finish my dinner. Perpetually “hangry” (hungry and angry), I was the Tasmanian devil of snacking, vacuuming up whatever food substances crossed my path, leaving wrappers and crumbs in my wake. “Never get between Talia and her food,” my brother facetiously coined when, like a voracious bull, I would bully my way into the kitchen to fix myself an emergent after-school snack. From the moment I was born, it seems, going more than two hours without eating was a physical impossibility. “I’m sick with hunger,” I would complain whenever my blood sugar levels dipped.
Now I sit here writing this article, in my adult incarnation, comfortably having abstained from eating for more than 14 hours. Whereas before I couldn’t go more than 2 hours without some kind of sugary snack, my body is now adapted to thriving during prolonged periods without food—and I feel all-the better for it.
“Eat a snack every 2-3 hours to keep blood sugar stable and lose weight,” dieticians and nutritionists often advise . However, as we dig into the disease prevention, anti-aging and weight management research, we learn that there may be benefits to going without food for prolonged periods.
We humans spent much of our evolutionary history hunting and gathering with extended periods of food scarcity. Our bodies adapted to survive through, and perhaps even thrive and depend on, periodic fasts. We now live in a society that enjoys food abundance: with 24-hour convenience stores and fast food restaurants at our disposal, we rarely go hungry. This recent lifestyle change may contribute to the increase in the diseases of excess that afflict modern bodies.
Ancient healing systems like Ayurvedic medicine and Traditional Chinese Medicine have long recognized the benefits of fasting for purifying and healing the body. Today, a body of research is accumulating that suggests that fasting may help treat diseases like multiple sclerosis and cancer, reduce the risk of chronic metabolic diseases, such as diabetes, battle dementia and cardiovascular disease, and reverse the effects of aging, helping us live longer.
What Happens During Fasting:
Human physiology fluctuates between two modes: the fasted and the fed state. After eating, a hormone called insulin rises in response to the intake of dietary carbohydrates and, to a lesser extent, protein. Insulin allows glucose to enter cells where it can be used for energy. Insulin encourages the storage of body fat and glycogen—a molecule stored in the muscles and liver that can be broken down quickly for energy. Insulin is an anabolic hormone that promotes tissue building and growth.
Our bodies are in the fed state, or postprandial state, for up to 4 hours following a meal, when blood sugar and insulin levels rise and the body begins to store food energy. 4-6 hours after eating, our bodies enter the post-absorptive state. Insulin and blood sugar levels fall, and blood sugar is maintained through the breakdown of liver and muscle glycogen. At the 10-12 hour mark post-meal, the body enters the fasting state. At this stage, glycogen stores have been depleted and blood glucose is maintained through a process called gluconeogenesis: glucose is created from fat, lactate and protein. In the fasting state, the body taps into fat stores to create ketone bodies, which are used for fuel.
Approximately 24-48 hours after a meal, the body enters a state called autophagy (or self-eating). The body breaks down old, damaged cells into their proteins and reuses them to build new cells or for fuel, through gluconeogenesis. Autophagy has gained the attention of researchers who recognize its benefits for managing inflammation, slowing the effects of aging, and treating various chronic diseases, such as autoimmune disease and cancer—more on this later!
Fasting to Treat Cancer:
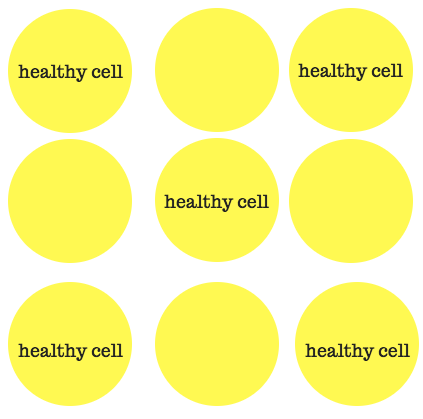
Valter Longo, PhD, at the Longevity Institute at the University of Southern California, examined the effects of 2 to 4-day fasts on patients with cancer who were undergoing chemotherapy. The study found that several days of fasting improved the efficacy of chemotherapy, while reducing its side effects, protecting healthy, non-cancerous cells. Healthy cells responded to the periods of food restriction by shutting down, protecting them from the toxicity of the chemotherapy. Cancer cells don’t have such a response, leaving them susceptible to the chemotherapy. “Cancer cells are dumb cells,” says Dr. Longo.
The fasting period not only improved the effects of cancer treatments, it stimulated the regeneration of the immune system through the creation of progenitor stem cells. Fasting cleared out damaged immune cells and cancer cells through autophagy and new cells were regenerated upon re-feeding. Dr. Longo and his team found that up to 40% of the immune system is rebuilt in mice after a fasting and re-feeding cycle.
Fasting Mimicking Diets:
Recognizing the difficulty in going 3 days without food, Dr. Longo developed a 5-day “Fasting Mimicking Diet” that allows for the consumption of about 700-1000 calories per day in the form of small snacks. The Fasting Mimicking Diet is low enough in calories, protein and carbohydrates to mimic the physiological conditions and benefits of fasting like autophagy, ketone body production, beneficial stress response, and cancer cell starvation.
Mice given the Fasting Mimicking Diet (FMD) lost 30% of their body weight through the breakdown of body fat and clearing away of old, damaged cells. When the mice were re-fed, their blood, brain and bone cells were rebuilt. The mice who underwent the Fasting Mimicking Diet had rejuvenated immune systems, decreased incidences of cancer, reduced body fat, improved cognitive performance, decreased inflammation, and increased lifespans.
Fasting to Treat Autoimmunity:
Research in mice showed promising results in using the Fasting Mimicking Diet to treat multiple sclerosis, a debilitating autoimmune condition that attacks the nervous system. When following the diet, immune cells that were attacking the brain and spinal cord were destroyed. Upon re-feeding, new progenitor stem cells were created that repopulated the immune systems of the affected mice, and aided in repairing the damage to the brain and spinal cord. The Fasting Mimicking Diet resulted in a 20% reduction in autoimmunity in mice with multiple sclerosis.
A study that examines the effects of the Fasting Mimicking Diet on humans with Crohn’s Disease, an autoimmune disease the affects the digestive system, are currently underway.
Fasting to Reverse Aging:
Autophagy, the process of removed and recycling old and damaged cells, is a new area of research for reversing the effects of aging. Autophagy alleviates the body burden of senescent cells that have stopped dividing but are still robbing the body of essential nutrients and energy.
When cells become senescent, they release inflammatory mediators, which can damage neighbouring cells and cause inflammation and disease. Cellular senescence is thought to be one of the primary mechanisms by which we age. As we age, more cells become senescent, causing age-related inflammation. A study found that inflammation is the primary factor that drives the aging process, damaging DNA and contributing to various diseases, such as cardiovascular disease, diabetes, arthritis, cancer, and autoimmunity.
The process of fasting and re-feeding stimulates the production of new, healthy progenitor stem cells in the immune system. Mice and human volunteers who underwent cycles of the Fasting Mimicking Diet had decreased numbers of myeloid cells, the inflammatory immune cells that become more numerous as we age, and increased numbers of cytotoxic T cells, which protect the body against viruses and cancer.
Fasting promotes longevity through its inhibition of Insulin-like Growth Factor -1 (IGF-1), a growth factor that promotes cellular growth, and prevents the death of senescent cells. Growth factors are important for growing babies and children, developing fetuses, boosting muscle, and growing new brain cells. However, growth factors like IGF-1 are negatively associated with longevity because of their potential to stimulate the growth of cancer and prevent autophagy. Mice whose growth factor-dependent genes were removed, or “knocked out”, lived 40-50% longer and suffered from less diseases as they aged. IGF-1 is stimulated by protein and carbohydrate intake; it is elevated in the fed state and inhibited when fasting.
Healthy humans who underwent cycles of the Fasting Mimicking Diet had lower risk factors that were associated with cardiovascular disease and diabetes, such as lowered blood pressure, reduced CRP (a marker of inflammation in the blood), and reduced fasting blood glucose levels. These markers remained improved even after the subjects returned to a normal diet, which indicates that fasting may help reduce the risk of chronic diseases, such as diabetes and heart disease, promoting health longevity and increased lifespan.
Fasting for Energy and Resilience to Stress:
Hormesis is the process in which the body’s response to a stressor like the slightly toxic flavonoids in plants, intense exercise, or extreme temperatures, benefits the body as a whole. Hormesis is one of the reasons that exercise and green leafy vegetables are so good for us; they impose minor stressors on the body, boosting its healing properties, and improving resilience.
Fasting, in addition to other positive stressors, up-regulates a stress-response gene called FOX03. When FOX03 is activated, it produces proteins that reduce inflammation, increase anti-oxidant production, repair DNA, and increase cellular energy production through the creation of new mitochondria. Humans with a more active version of the FOX03 gene have an almost 300% chance of living to be over 100 years old.
Fasting also promotes a process called mitophagy. Similar to autophagy, mitophagy involves removing and recycling damaged mitochondria that are no longer able to effectively produce energy. Through activation of the FOX03 gene, more mitochondria are created to replace the old, improving energy production. The creation of new mitochondria only occurs in response to exercise, extreme temperatures, and periods of fasting.
Fasting for Weight Loss:
It doesn’t take a researcher to figure out an obvious truth about fasting: when you don’t eat, you lose weight. Dr. Jason Fung, MD, a Toronto-based nephrologist, prescribes fasting to his obese and diabetic patients. In his book, The Obesity Code, Dr. Fung discusses how the old paradigm of restricting calories for weight loss—eating 1500 calories a day while burning 2000, for example—is out-dated and ineffective for keeping weight off longterm. Dr. Fung argues that fat storage and breakdown are not the result of a simple calories in minus calories out equation, but the performance of a hormonal orchestra conducted by insulin. Insulin stores fat and glycogen, while inhibiting the release of fat breakdown. The body only begins to tap into its glycogen and fat stores when insulin drops during the post-absorptive and fasting phases after a meal. Once it depletes its glycogen stores, the body burns fat as its main source of fuel as long as insulin levels remain low.
According to Dr. Fung, fasting is superior to caloric restriction diets because it keeps insulin levels low for long enough to allow the body to deplete its glycogen stores and tap into fat. Fasting also releases surges of growth hormone, which prevents muscle loss, and norepinephrine, which boosts energy and feelings of well-being. Unlike caloric restriction diets, studies have shown that metabolism increases during and after fasting, preventing weight regain. Dr. Fung argues that fasting can spare muscle, boost metabolism, increase energy, and increase feelings of well-being, making it an effective tool for lasting weight loss.
Ways to Fast:
While the health benefits may be numerous, fasting isn’t easy. The first time I tried a prolonged fast, all I could think about was food. Food was everywhere and the people around me seemed to be eating all the time. My body, accustomed to being constantly fed, wasn’t too happy with the sudden metabolic switch I was demanding from it. Many of our metabolisms have been trained to run on dietary carbohydrate and glycogen as their primary fuel sources, making the first few hours to days of fasting a challenge. However, there are many ways to ease into the practice of fasting. You can obtain Dr. Valter Longo’s Fasting Mimicking Diet kit from a healthcare provider through ProLon, or practice small intermittent fasts, such as Time-Restricted Feeding.
Time-Restricted Feeding:
A researcher at the Salk Institute in Califoronia, Dr. Sachin Panda, PhD, found that restricting eating time had amazing health benefits in mice. Mice were fed an unhealthy diet of lard and sugar. The mice, as you might expect, had shorter lifespans and a variety of health problems: diabetes, obesity, and heart disease. However—and this part is miraculous—when Dr. Panda and his team restricted the time the mice were fed the exact same crappy diet to 12 hours (instead of allowing them to eat whenever they wanted), none of the negative health benefits occurred; the Time-Restricted Fed mice were 70% leaner, lived longer and were free from diabetes or heart disease.
Further investigation revealed that restricting feeding time to 8-12 hours a day, resulted in mice that had less body fat, improved muscle mass, decreased inflammation, increased cardiovascular function, increased mitochondrial function, higher levels of ketone body production, increased cellular repair processes and anti-oxidant production, and increased aerobic endurance. It was when the mice ate, not what they ate, that conferred these health benefits.
North Americans, on average, eat on a 15-hour clock. We seem to eat constantly, stopping only to sleep. To study the effect of Time-Restricted Feeding on humans, Dr. Panda had human participants restrict their food intake to 12 hours a day; if the volunteers had their first sip of coffee at 7 am, they were told to cease all food intake by 7pm. After the completion of the 16-week study, the volunteers lost 3-5% of their body fat without making a conscious change to their diets. The participants reported sleeping better and feeling more energized in the morning. They noted that their overall calorie consumption decreased by about 20% without effort.
Research into Time-Restricted Feeding indicates that allotting at least 12 hours a day to fasting boosts the body’s repair mechanisms, improves digestive function and motility, provides time for the body to switch to ketone body production (which tends to happen 10-12 hours after a meal), improves blood sugar control, regulates appetite, and enhances stress resilience. Taking a break from eating allows the body to invest its energy into repair, rather than digestion. The best part about Dr. Sachin Panda’s research is its simplicity; to obtain all of the benefits, simply avoid after-dinner snacks!
Intermittent Fasting:
Similar to Time-Restricted Feeding, Intermittent Fasting plays with the ratio of fasted to fed hours. Proponents of Intermittent Fasting refrain from eating from 12 to 23 hours within a 24-hour period. A common ratio of fasted to fed time is 16 to 8 hours: fasting for 16 hours a day and eating within an 8-hour window. For example, if breakfast is at 8am, then those following a 16:8 intermittent fast stop eating by 4pm in the afternoon.
Alternate Daily Fasting or the 5:2 Diet:
Studies with mice and human subjects found that alternating daily food intake, or following a 23:1 fast (having just one meal a day) every second day, was effective for weight loss. The protocol is beautifully simple: every second day either fast completely or indulge in only one meal. While people tend to eat more on their “fed” days, they don’t seem to make up the calories that are lost on the fasting days, resulting in an overall reduction in calories and weight loss.
Water Fasts:
It’s estimated that we need to fast for at least 36 hours to get the autophagy benefits, which makes water fasting a powerful therapeutic and anti-aging practice. Water fasting is simple: withstand extended periods, usually 3 to 5 days, but often longer, only consuming water.
The longest recorded water fast was 382 days, performed in 1973 by a 27-year old male who weighed 456 lbs. During the months he fasted, the 27-year old consumed only water and a multivitamin and, according to the study published on him, experienced “no ill-effects”. While water fasts can have amazing therapeutic benefits, it is advised that they be medically supervised.
Ketogenic Diets:
Ketogenic diets are high-fat diets that restrict carbohydrates and limit protein, and can mimic the low-insulin conditions of fasting. Because carbohydrates and protein are restricted, the body is forced to turn dietary fat into ketone bodies, which it can use for energy.
Ketone bodies, especially beta-hydroxybutyrate, produced from either dietary or body fat, have important therapeutic uses. They provide more energy for the brain than glucose, which can have benefits for memory, mood, concentration and cognitive performance. Ketogenic diets have been recommended for treatment-resistant epilepsy, and diseases associated with cognitive decline like Alzeimer’s and Parkinson’s. More recently ketogenic diets have been recommended for mental health conditions, such as depression and anxiety.
Ketone bodies also help cells resist oxidative stress, preventing cellular damage, which makes ketogenic diets of interest to cancer researchers because or their ability to starve cancer cells of protein and carbohydrates, while fuelling healthy cells.
Ketogenic diets can deliver many of the benefits of fasting because of the low-insulin, low growth factor conditions they induce. When a person becomes “keto-adapted”, able to burn ketone bodies efficiently for fuel, the transition to fasting is easy. For this reason, ketogenic diets and fasting often go hand-in-hand.
Cautions:
While fasting can deliver many health benefits, it can impose a temporary stress on the body for those who haven’t adapted to ketosis or prolonged periods without food. Therefore, it’s important to fast under the supervision of a medical professional, especially if deciding to embark on an extended fast.
Before deciding to fast, the individual’s energy levels and vitality, health status, hormone regulation (those who are taking insulin should practice extreme caution when fasting), age, health history, and health goals, should all be considered. A woman of fertility age will have different health goals than a 72-year old woman with type II diabetes. The former may want to preserve body fat and promote fertility and ovulation, while the latter may want to reduce her insulin and growth factor levels, and lose weight in order to promote health longevity.
Fasting may not be appropriate for everyone. For example, those who are underweight, pregnant, breastfeeding or suffering from an eating disorder should not fast. Fasting in women of reproductive age has the potential to produce hormonal imbalances such as hypothalamic amenorrhea (irregular or absent menstrual cycle). Fasting can exacerbate or cause dysregulation in stress hormones, particularly cortisol, known as “adrenal fatigue”, and potentially effect thyroid function, as a result of the body’s starvation response. Fasting while under the pressure of chronic mental and emotional stress is probably not a good idea. Working with a professional and listening to your body are key elements to doing fasting right.
However, when used correctly, it can be a simple, free, powerful therapeutic tool for healing the body, treating chronic disease, and promoting longevity.
Sigh… I just finished reading a rather annoying article in the Globe and Mail (don’t even bother to click and add more Google street-cred, seriously) that doesn’t really warrant a response but… here we go. It’s my day off.
The article was written by one Carly Weeks, who doesn’t seem to have a very positive view of naturopathic doctors. I don’t know Carly and have no idea about her health history, but I’m going to take a shot in the dark and imagine she hasn’t suffered from chronic eczema.
Let me know how that steroid cream works out for ya, Carly!
But, ad hominem aside, her issue with naturopathic doctors this week(s)—pun intended, aren’t I hilarious—is, what else: we’re a bunch of quacks who use nothing but false therapies and smooth-talking to coax our patients into thinking they feel better. Well, if that worked, I wonder why more healthcare practitioners don’t try copying those moves too. It might save the government some money, which is what, coincidently, naturopathic medicine is already doing and it’s not by false therapies and smooth-talking. (But we do make time for a lot of talking).
The Globe piece begins with a story about how physicians (not naturopaths, for the record) prescribed radioactive water in the 1920’s. It’s a cute and tragic story about limited safety profiles. And other than its juxtaposition in an article about NDs, I’m not sure what the writer’s point was. We don’t use radioactive water to treat anyone. If you want radiation, which is a therapy, a cancer treatment, then you must see an oncologist. Talk about throwing out babies and bathwater.
The article is largely about how naturopathic doctors are moving under a new regulatory board, under the Regulated Health Practitioners Act. This limits our scope compared to that of provinces like BC or certain US states, where naturopathic doctors have been prescribing drugs and even performing minor surgeries safely where it’s warranted.
Here are some facts:
Naturopathic medicine is incredibly safe. We are trained in conventional diagnosis, anatomy, physiology, physical exams, including gynaecological exams, breast exams and digital rectal exams. We have the ability to perform acupuncture in Ontario and give intramuscular injections. With additional training we can provide IV treatments. We are trained to order and interpret labs and to take blood. I will not deny that conventional medicine and pharmaceuticals have saved millions of lives. However, we know that 10,000 yearly deaths in Canada (and 100,000 in the US) are due to pharmaceuticals alone. A year ago I wrote a post talking about the off-label birth control pill Diane-35. Let’s not start comparing safety profiles here.
Naturopathic doctors are highly trained and educated: We have completed a 4-year very rigorous program that includes a 12-month internship where we treat patients in an out-patient facility. In our training we performed over 100 practical and written examinations. After our second and fourth year we complete two licensing exams, which span a course of 5 full days of examinations combined. Ask anyone I know if what I did was easy. Trick question: they wouldn’t know because they didn’t hear from me for the past 5 years–I was studying the WHOLE time. It’s ok, though, because now I know a lot.
Naturopathic medicine is a regulated profession: In order to practice in Ontario naturopathic medical graduates who have passed both licensing exams, must pass a series of board examinations that are both written and practical. We then must enter into a month-long application process, which includes a police background check and character reference check. If I try to delay treatment of an emergent condition or treat an emergent condition with something like homeopathy or acupuncture (effective treatments for other conditions, but not emergent, life-threatening ones), which is something we are often accused of potentially doing, my licence will be removed. It’s not something we do—it’s that simple. We are held accountable and have a lot of responsibility to deliver safe care.
Naturopathic doctors are health experts: In order to complete the naturopathic medical program we complete 1200 hours of clinical training and 3000 hours of classroom training. This does not include study time for our board exams and pursuit of side interests or continuing education credits that are required to maintain licensure. We are trained in nutrition, which many medical professional, including medical doctors, are not. Naturopathic doctors often see patients that have been failed by the conventional medical system, which means we deal with complex cases on a regular basis. This demands that we keep our skills sharp and our knowledge current.
Naturopathic medicine provides the public with an amazing service that patients are willing to pay for: We spent up to two hours at time with our patients, educating them on any topic of their health picture: the medications they’re on that their doctors don’t have time to discuss with them, their health conditions, their prognosis and what else they can do about it. I spent half an hour talking about an STI a patient of mine had been diagnosed with. She’d seen two doctors and a specialist. None of them had talked to her about it. Patients have told me their doctors no longer perform physicals. Well, we do. And, it turns out, people pay for excellent care. Naturopathic medicine provides the much-needed service of patient education, human-centred care and prevention of disease. It’s an excellent complement to an effective whole-person healthcare strategy.
Naturopathic medicine works: I could say more on this but let’s keep it brief: if it didn’t work, people wouldn’t pay for it. The Globe and Mail, more than anyone should know to “let The Market speak.” (Amiright?) I lied, I will say more. If you don’t think naturopathic medicine works, then call my patients who no longer have chronic pain or allergies or chronic constipation. Ask my patient who couldn’t conceive how her daughter is doing. Blah blah, we help people.
Naturopathic doctors prefer to work in collaboration with other healthcare professionals: Ideally each patient should be managed by a healthcare team. When I start seeing a new patient I immediately establish a relationship with his or her medical doctor. I refer out for labs and to specialists if necessary. Medicine should be integrative, not alternative. Patients shouldn’t be forced to choose.
In addition to accusing us of being a bunch of unsafe quacks, the author writes, “Ontario should have created a regulatory system based on the principle of evidence first.” So, there you have it. Only medicine that is based in evidence should be regulated by the province.
Wow, what a ridiculous statement made by someone who I imagine knows little to nothing about how medicine and so-called “evidence” works.
Firstly, there is more than one type of evidence. In fact, evidence is a hierarchy. At the bottom we have things like clinical case reports or expert opinion, what my friends the skeptics love to call “anecdotal evidence.” Sigh. If you’ve seen something work, you keep doing it. It’s not the best evidence we have, but it’s still evidence. The better forms of evidence, randomized control trials, are being done on naturopathic therapies and naturopathic therapies have been found to hold steady. Actually, many of the therapies we prescribe are done precisely because there is evidence to support it: fish oil for depression and bipolar disorder? Inositol for fertility in patients with PCOS? Evidence, evidence, evidence.
Secondly, only 10% of medical guidelines are based on the type of “evidence” that our friend Carly Weeks is likely referring to: the Randomized Control Trial, which involves comparing two groups: a treatment group to an inactive group that gets something like a placebo. Well, it turns out, we just don’t have that much “evidence” of this sort to dictate what happens in medicine. A tourniquet for a bleeding wound? Using general anesthetic rather than nothing? These things haven’t been compared against placebo. What is the other 90% of medicine based on? Expert opinion: a nice mixture of clinical expertise, intuition, common-sense, “what the heck, might as well try it it couldn’t hurts” and research. I don’t see Carly questioning the use of SSRI for mild and moderate depression or beta-blockers to prevent cardiac events as a result of high blood pressure, both of which have “no evidence” to support their use. Nope, just crickets when it comes to those topics.
Thirdly, the father of EBM, or Evidence Based Medicine, himself, Dave Sackett, said, “Good doctors use both individual clinical expertise and the best available external evidence, and neither alone is enough. Without clinical expertise, practice risks becoming tyrannized by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient.” (Emphasis mine). Individual clinical expertise from both modern and traditional medicine, the best available external evidence and tailoring treatments to individuals patients needs and preferences? Sound like naturopathic medicine to me.
Naturopathic medicine is safe and effective. We have a patient-centred approach and offer wonderful service for the cost, which is often covered by insurance benefits. Naturopathic doctors take the time to listen to your story and educate you on what is happening in your own body. We treat the root cause of your condition, rather than masking symptoms. We are highly-trained healthcare professionals and we are regulated. Soon we will be moving to different regulation. However, the government will be removing some of the rights we’ve had, which include ordering certain lab tests that we’ve safely ordered for years. If you use or support naturopathic medicine, please click the link to sign the petition to maintain the current naturopathic scope of practice in Ontario and support safe and effective natural healthcare for all Ontarians.
Green tea, from the tea plant Camellia sinensis, with it’s metabolism-boosting, antioxidant and anticancer powers is now expanding its talents, entering into the world of skin care, especially acne treatments, and experiencing great success.
When I was very small, the tree at my parent’s house became sick and was cut down. I don’t exactly remember the great pine tree, but I remember it’s large, rotting stump, which was left as evidence of its towering existence on the lawn of our front yard. As a replacement, the city planted another tree in its place: a ginkgo tree.
What was once a disappointingly small, skinny sapling now towers over the two-story house, its trunk the diameter of my outstretched arms, an alarming reminder of the passage of time. I have always been fond of our ginkgo tree, with its delicate, fan-shaped leaves and its aire of exoticism, but I am developing an entirely new relationship with the plant as I begin to discover its array of clinical uses as well.
The new year brings with it the onslaught of new year’s resolutions, the most common being, of course, to lose weight. While most people think that losing weight can help them better their health and well-being, a new study published in JAMA begs to differ.
It seems that, for every person who embraces the idea of holistic medicine with open arms and an open mind, there is at least one skeptic who refuses to acknowledge that alternative medical practices not only exist, but are growing in popularity, helping thousands of people and, most likely, are here to stay.