I, like most of my colleagues became a naturopathic doctor because of my own extremely disempowering experiences with the healthcare system.
In my late teens and early 20s I was suffering from what I now know were a series of metabolic and hormonal issues and I, like almost all of my patients and colleagues experienced confusion, gaslighting, frustration and a complete lack of answers for what I was dealing with. I tell my story more in depth in other places, but I was told to “stop eating so much”. I was told everything was normal in bloodwork (or simply not called back). I was weighed incessantly. I was chastised for doing my own research (I had to–no one would tell me anything). I was interrupted, cut off and dismissed.
And so, I did what most of my colleagues do–I got educated. I went to school. First for biomedical sciences and then, when that degree left me with more knowledge gaps than answers (and no one who would indulge, let alone answer, my questions), I became a naturopathic doctor.
Throughout my 8 years as a practicing ND, I have encountered thousands of similar stories of disempowerment and confusion and frustration. We patients are trained to see our doctors when we feel depressed, fatigued, or debilitated by PMS, menstrual pain, headaches, and mood issues. Most of us don’t care what answer we get–fine, if it’s a medication I need, I’ll take it! But if we experience lack of benefit from the solutions and a lack of answers, then what? I’ve heard this story over and over.
And so, like many of my colleagues I use the privilege of my education to help me navigate the system. I ice a sore foot for 2 days and then get an x-ray (picking a non-busy time to visit the ER). I take the orthopaedic surgeon’s advice with a grain of salt and implement my own strategies for bone healing. I ask for the bloodwork I need (and know my doctor will agree that I need) and pay for the rest out of pocket. I know my doctor’s training and I understand her point of view and I don’t get frustrated when diet and nutrition or lifestyle are never mentioned. I don’t get upset if my doctor doesn’t have an explanation for symptoms that I now know are related to functioning and not disease, and that it is disease which she is trained to diagnose and prescribe for.
And thankfully, my experience with the healthcare system has been quite limited as I’m able to treat most things I experience at home and practice prevention.
My good friend, who is a naturopath as well, and who has given me permission to share her story, had the same experience up until this summer. She too used the healthcare system quite judiciously and limitedly until a series of stressors and traumas landed her in in-patient psychiatric care (i.e.: a psychiatric hospital) for a psychotic episode–her first.
…And until she started experiencing debilitating gastroesophageal symptoms that were beyond what one might consider “normal.”
And in both cases she sought help from the medical system. She told me recently that her experience was quite different from the ones she’d had in her 20s when her long-standing parasite was misdiagnosed as IBS and she was repeatedly dismissed by doctors. She told me “I’ve been having great experiences with the healthcare system. It’s not like it was before. My doctors have listened to me. They’ve been helpful. Yes, they’ve recommended drugs but when I tell them that I don’t want to take the medications because I know what they do and how they work and don’t think I need them, they respect that. They treat me like I’m a real person. They’re all our age, too. The procedures are more state-of-the-art. The facilities are pleasant. Something has changed in healthcare.”
I know that my friend’s experience might be different from yours. I’m not saying her experience is universal. In fact, if I reflect on my interactions with the fracture clinic in St. Joe’s hospital in Toronto, I had a fairly good experience as well (except for long wait times and booking errors). Sometimes medical trauma can blind us to reality–sometimes we aren’t willing to re-evaluate our assumptions until someone points out a piece of reality that is hard to deny. I actually haven’t had a direct negative experience with healthcare in years– and yet I had chalked that up to the fact I rarely need to use it.
But my friend had had two quite intense experiences and came away from them feeling positive about the care she received. I wondered what was different. Here are my thoughts.
Medical care has evolved. It is inevitable that this happens. Sometimes we might have just had a bad doctor, or someone who was having a bad day or maybe was triggered by our experience. I sometimes think not knowing how to help triggers doctors—I think this might have been the case with the doc who told me to eat less. She might have felt helpless and incompetent at not being able to help me and projected those feelings onto me as a “difficult patient”.
Ultimately health professionals got into their field to “help people”. If you’re not helping people you might feel triggered. But then, if you’re a competent professional, and I believe most are, you look for new ways to help. You open your mind to other practitioners, like NDs. You might not understand why or how what they do works, but “whatever works.”
Doctors are increasingly open to new studies on nutrition. They recognize treatment gaps in their care and in medical knowledge and guidelines. Nutrition and alternative practices are entering mainstream and are dismissed as “woo woo” less and less, particularly by doctors who embrace science and research.
With the evolving landscape of medical care, doctors and health professionals are adapting to new perspectives and approaches to help their patients effectively. Acknowledging that some past encounters might have been influenced by various factors, professionals are increasingly open to alternative practices and unconventional methods. They are embracing the significance of research and scientific advancements, often exploring innovative solutions such as the MAS Test to bridge treatment gaps and enhance patient care. By incorporating cutting-edge tools like the MAS Test, doctors are demonstrating a commitment to understanding diverse approaches, ensuring they provide comprehensive and personalized healthcare solutions to their patients. This openness to holistic methods and ongoing research not only enriches medical knowledge but also fosters a more inclusive and effective healthcare system for everyone.
I always say, when picking a doctor pick one that listens, that is curious and that is humble. I strive to be these things, although it’s not easy. Practicing medicine is as much an art as it is a science–we need to be able to not only admit but carry with us the absolute truth that we do not know everything. It is literally impossible to know everything. The body and nature will constantly present us with mysteries on a daily basis, but the gift of being a clinician is that we are constantly learning.
“I don’t know, but I will try to find out” should be every doctor’s mantra (along with Do No Harm).
In a busy and overloaded system we need to help healthcare workers help us. This means being informed. My friend is highly informed and educated in healthcare. I believe her healthcare providers could sense this. She was respectful in denying medications and wasn’t pushed (because she had informed reasons that the healthcare practitioners ultimately agreed with, “no, you shouldn’t go on a PPI long-term, that’s right” “yes, anti-psychotics do have a lot of side effects, and taking them is a personal choice”).
A significant element of my medical trauma was the feeling of disempowerment. I was completely in someone else’s hands and they were not communicating with or educating me. I was left feeling lost and hopeless. Empowerment is everything. It allows you to communicate and make decisions and weigh options. You know what healthcare can offer you and what it can’t.
Of course we can’t always be empowered, especially when we’re very sick and when we’re suffering. In this case, having advocates in your corner are essential. Perhaps it’s having an ND who can help you navigate the system, think clearly and help you weigh your options.
I also recognize that it is hard to be empowered in emergencies. Fortunately, modern medicine handles emergencies exceptionally well. Still, in this case, having an advocate: friend, practitioner or family member, is an incredible asset.
Physicians are burned out. Patients are burned out. I believe this is because of responsibility. Neither the medical system nor the individual can possibly be solely responsible for your health. I believe that responsibility is better when shared. We need help. We can’t do things alone: we need someone’s 8+ years of education, diagnostic testing, clinical experience and compassion. We also need our own sense of empowerment so that doctor’s don’t succumb to the immense pressure of having to fix everyone and everything.
My sister in law is an ER nurse and once remarked (when asked if the ER was busy and chaotic) “people need to learn self-care”. She didn’t mean self-care as in bubble baths. She meant: learning how to manage a fever at home, when a cut needs stitches or how to determine if a sore ankle is a sprain, strain or break. A lot of people were coming in with colds—self-limiting, non-serious infections that could easily be treated at home. This was burning her out. Of course, she meant, go to the ER if you’re not sure. But, there are many non-grey areas in which we can feel empowered to manage self-limiting, non-serious health conditions as long as we know how to identify them or who to go to for answers.
Education is power. In a past life (before becoming an ND and while studying to become one) I was a teacher. I am still a teacher and in fact the Latin root of the word doctor, docere, means “to teach.” Healthcare is teaching. No doctor should say “just take this and call me in the morning” and no patient should accept this as an answer. We have the right to ask, “what will this pill do? When can I stop taking it? How does it work?” This is called Informed consent: the right to know the risks and benefits of every single treatment you’re taking and the right to respectfully refuse any treatment on any grounds.
You have the right to a second opinion. You have the right to say, “Can I think about this? I’d like to read more about it.” You have every right. You have the right to bring a hard question to your doctor, like “do I really need this statin? A study in Nature found that the optimal cholesterol level for reduced all-cause mortality is around 5.2 mmol/L, which is much higher than mine. Do I really need to be on something that lowers my cholesterol?”
If we can’t speak to our doctors, we turn to Google. Being a good researcher is a skill. This is what I was trained to do at naturopathic medical school and in undergrad. How can you tell if a study is a good study? Does the conclusion match the results? What does this piece of research mean for me and my body? Your doctor should be able to look at you and answer your questions to your satisfaction. This is basic respect.
You deserve to access the results of your blood tests and be walked through the results, even if everything is “normal”. Even a normal test result tells a story. We deserve transparency.
I was once told in a business training for healthcare practitioners (NDs, actually) that “people don’t want all the information. They don’t want to know how something works. They just want you to tell them what to do.”
Now, I sincerely disagree with this. In my experience, patients listen vividly when I walk them through bloodwork, explain what I think is happening to them and try to describe my thought process for the recommendations I’m making. I’m sure a lot of what I say is overwhelming–and then I try to put it differently, and open the conversation up to questions to ensure I’m being understood. Again, doctor as teacher, is a mantra we should all live by. There are few things more interesting than learning how our bodies work. In my experience, patients want to know!
When our bodies occur as a mystery, we are bound to live in fear. We are bound to feel coerced and pressured into taking things that our intuition is telling us to wait on, or seek a second opinion for. When we are scared to ask our doctors questions or take up their time, we end up having to deal with our concerns on our own. When we are dismissed we end up confused and doubting ourselves. We end up disconnected from our bodies. We are anxious. We catastrophise. We give away our power to strangers.
Empowerment is everything. It helps us connect to our bodies. It strengthens our intuition. We know where to go or who to go to for answers (or at least a second or third, opinion). We can move ahead with decisions. (i.e.: “I’m going to take this for 8 weeks and if I don’t like the side effects, I will tell my doctor that I want to wean off or ask for another solution”). We are aware of the effects and side effects of medications. We are aware of our options. We know if something isn’t right for us. We can make food and life style choices in an informed and empowered way. We can feel in our bodies who is trustworthy. We can trust ourselves and our bodies.
When patients are empowered, I believe doctors experience less burnout. The responsibility is shared evenly among patients, friends, family and a circle of care of helpers. No one faces the entirety of the weight of their health alone. No one should.
Empowerment and health don’t mean that you’ll be completely free of disease, or that your body will never get sick, or that you will be pain and suffering free. We all get sick. However, empowerment can help you notice something is off. Increased awareness helps you advocate for yourself to get the care you need in a timely fashion. It helps you take necessary steps, even if you’re afraid. You might be less afraid when you have more information. You might have more hope when you know all your options.
Empowerment in healthcare is everything. And here’s the thing: your doctor wants you to be empowered. Empowered patients are fun to work with. They ask good questions. They are respectful. They are open. They give us practitioners an opportunity to learn. My friend experienced this. I’m sure she was a joy of a patient to work with because she was knowledgeable, alert and present. She maintained her own power. She asked questions when she was unsure. She knew what questions to ask. She knew where to go for answers on her own time. She knew which information was relevant for her practitioners to know. She knew how to ask for time and space before making a decision. She knew how to maintain her sense of autonomy. Most of all, empowerment gives us the strength to find a new practitioner if the therapeutic relationship we’re in isn’t respectful or supportive.
I believe we get into the helping professions to help–to heal, to learn and to alleviate suffering. We all swore an oath to “do no harm”.
What do you think? How has health empowerment helped you navigate your own healthcare?
We’ve been hearing quite a lot about The Science these days. So, what is science? How does science guide medical practice and naturopathic medicine?
The science council defines science as, “the pursuit and application of knowledge and understanding of the natural and social world following a systematic methodology based on evidence.” The answer is, science is a methodology.
It is applied in medicine through Evidence Based Medicine (EBM) which starts with the individual patient and incorporates: clinical expertise, scientific evidence (that best that exists according to a hierarchy), and patient values and preferences.
“Evidence medicine is the conscientious, explicit, judicious and reasonable use of modern, best evidence in making decisions about the care of individual patients. EBM integrates clinical experience and patient values with the best available research information.”
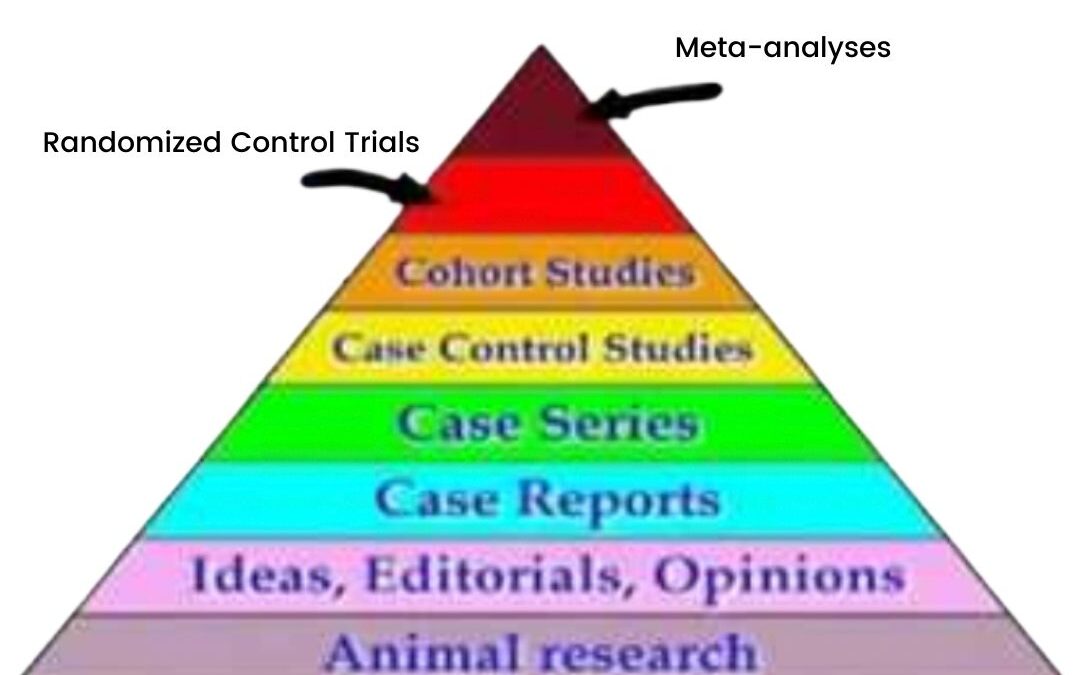
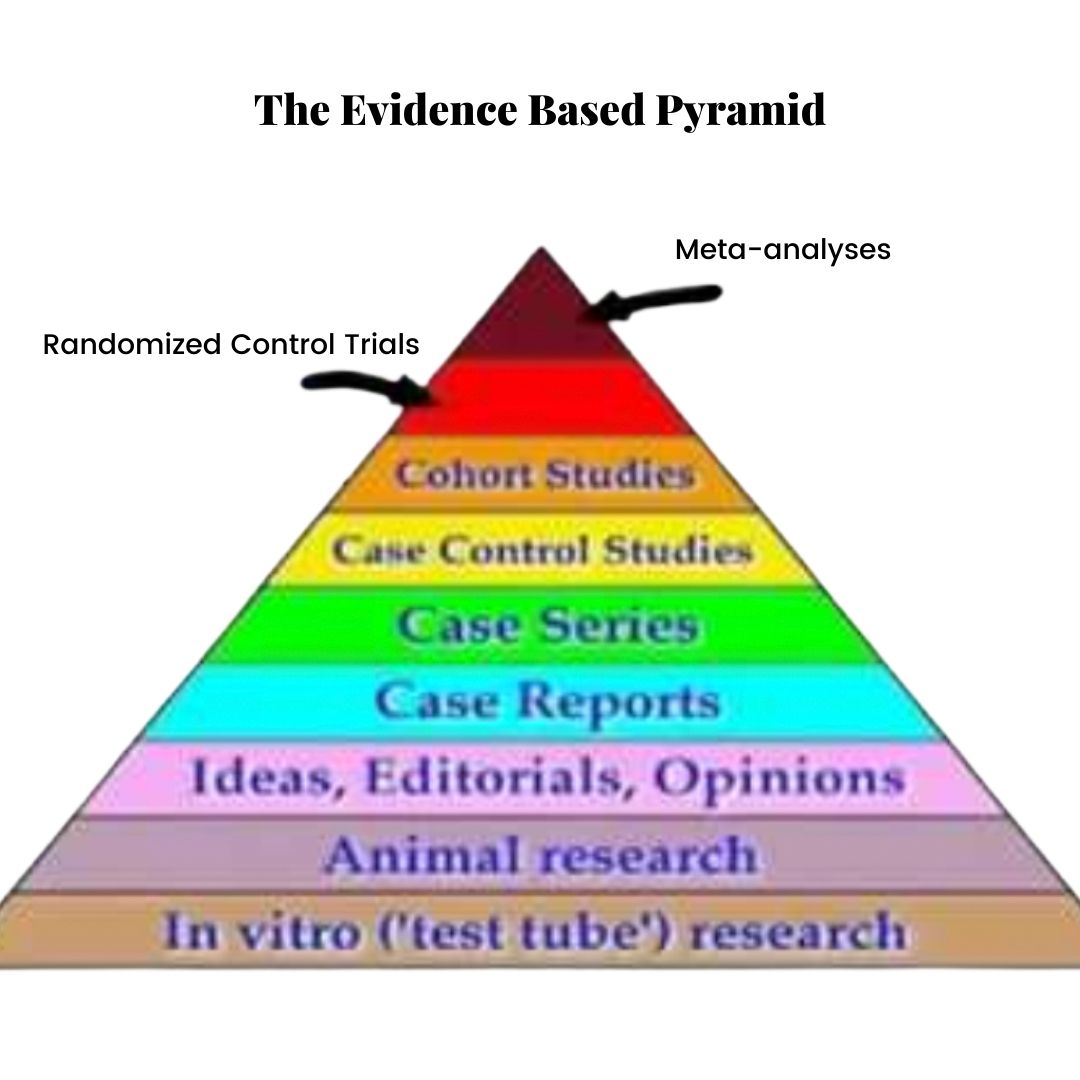
The Evidence-Based Pyramid
In EBM, evidence exists in a hierarchy, represented by the Evidence Based Pyramid (shown above). Animal studies are at the bottom, case reports (clinical anecdotes) somewhere in the middle and randomized control trials and meta-analyses (the Gold Standard of evidence) at the top.
Dave Sackett (the Father of EBM) et al. write in the British Medical Journal (1996),
“Good doctors use both individual clinical expertise and the best available external evidence and neither alone is enough.”
In addiction to scientific evidence, EBM must incorporate:
Patient values
A bottom-up approach (it is patient-centred, not guideline-centred)
The needs of the individual (EBM is not a one-size-fits-all formula)
Clinical expertise
The best available evidence: this does not mean using only randomized control trials. Sometimes the best evidence we have are case reports, historical and traditional use of an herb or animal studies. We still owe our patients the opportunity to see if a treatment works for them, especially if the risk of a given treatment is low.
As clinicians, we use our knowledge in different ways. We start with an assessment of the individual in front of us. This assessment takes into account the factors that influence this patient’s life, their lifestyle, their health condition and their overall health goals.
We then turn to clinical experience, research, our scientific knowledge and guidelines.
We share this information with our patient. Our job is to educate and convey the options so that the individual can provide informed consent. How does this knowledge fit into the patient’s life? How does it inform their choice?
Science is not a set of values. It is not a religion. We do not follow it.
Science provides us with a methodology for seeking the answers to questions we might ask about how the principles of nature, including the human body, are organized.
Science encourages us to ask questions and testing hypotheses in order to find answers.
It is never settled.
Most of all, science doesn’t tell us how to use scientific knowledge.
Our choices are governed by our goals, preferences and values.
So, “follow the sicence?”
No. Follow your goals, preferences, values and dreams.
And use science to help guide your way.
Reference:
Sackett, D. L., Rosenberg, W. C., Gray, J. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. BMJ, 312(7023), 71–72.
“The right to determine what shall or shall not be done with one’s own body, and to be free from non-consensual medical treatment is a right deeply rooted in Canadian common law. The right underlines the doctrine of informed consent.
“With very limited exceptions (such emergency use or incapacity), every person’s body is considered inviolate and accordingly every competent adult has the right to be free from unwanted medical treatment.
“The fact that serious risks or consequences may result from a refusal of medical treatment does not vititate the right of medical self-determination.
“The doctrine of informed consent ensures the freedom of individuals to make choices about their medical care. It is the patient, not the physician (or others) who ultimately must decide if treatment–any treatment–is to be administered.” Justice Robbins of the Ontario Court of Appeal.
I deeply believe that the key to optimal health is taking full responsibility and accepting all personal power for one’s own health. This may involve doing research, educating oneself, or assembling a team of trusted health professionals, with you, the patient at the centre.
We have a busy and overloaded healthcare system and even well-meaning professionals can find themselves hurriedly having a conversation in which they are not properly informing patients of the risks and benefits, or alternatives to treatment that they are recommending. I have had patients hurriedly scheduling for surgeries they weren’t sure they wanted, or pressured into hysterectomies or long-term treatments whose risks they didn’t understand.
I have also had patients make perplexing choices in the name of their own care–choices I didn’t necessarily agree with, such as forgoing conventional cancer treatments or further testing or screening.
However, it is the duty of the healthcare provider to provide advice. And it is the right of every patient to accept or reject that advice.
In light of recent, disturbing events, I have started posting some facts on Canadian law and Informed Consent only to be met with surprise–many people are not aware of their rights to refuse medical treatment, to be informed of the risks, and to be allowed to make a choice free of pressure or coercion.
Despite it being deeply enshrined in Canadian law, many patients are not aware of their right to full bodily integrity, autonomy, and choice.
Since 1980, the Supreme Court of Canada made it the right of every patient to be given full informed consent before any medical procedure such as taking blood, giving an injection or vaccination, performing a physical examination, exposing the patient to radiation, and so on.
“The underlying principle is the right of a patient to decide what, if anything, should be done with his body.” Is quote from the famous Supreme Court case of Hopp v. Lepp.
Every health professional under the Regulated Health Professions Act, including naturopathic doctors has a duty to uphold informed consent. We are well versed in it. We are required to uphold it, document it, and maintain it with every patient we see.
Our naturopathic guidelines on consent state, “The ability to direct one’s own health care needs and treatment is vital to an individual’s personal dignity and autonomy. A key component of dignity and autonomy is choice. Regulated health professionals hold a position of trust and power with respect to their patients and can often exercise influence over a patient; however, decision-making power must always rest with the patient.”
In 1996 Ontario passed the Health Care Consent Act, a legal framework for documenting, communicating, establishing and maintaining informed consent in all healthcare settings.
Informed consent is required before all treatment can be administered. Treatment includes: “anything that is done for a therapeutic, preventive, palliative, diagnostic, cosmetic or other health-related purpose, and includes a course of treatment, plan of treatment or community treatment plan.”
Informed consent must be present in 4 key areas:
The consent must relate to the treatment.
The consent must be informed.
The consent must be given voluntarily, i.e.: made by the patient, and under no coercion, pressure, or duress.
The consent must not be obtained through misrepresentation or fraud.
In order to obtain your full informed consent, you must be given the following information:
The nature of the treatment.
The expected benefits of the treatment.
The material risks of the treatment, no matter how small, especially if one of the risks of side effects is death. The risks should not be minimized for the purpose of influencing your decision-making. The risks should be in relation to your health history. For example, if you suffer from cardiovascular disease, you should be made aware of the the risk of blood clots or myocarditis. It should also be disclosed if certain risks remain unknown.
The material side effects of the treatment. Again, these side effects should be explicitly stated, no matter how small, and if long-term side effects are unknown, that should be stated.
Alternative courses of action.
The likely consequences of not having the treatment. These consequences should not be exaggerated and must be related to the particular patient at hand. What is the actual risk of the patient not receiving the treatment?
Consent cannot be given in a state of duress or coercion. Healthcare providers must be aware that they hold a position of authority and may maintain a power imbalance. They must not misrepresent the benefits of the treatment, and they must disclose any conflict of interest.
Healthcare providers must ensure that patients are not acting under the pressures of someone else, such as an employer, government agency or family member, and are making this decision on their own.
Finally,
The Informed Consent Guide for Canadian Physicians states, “Patients must always be free to consent to or refuse treatment, and be free of any suggestion of duress or coercion. Consent obtained under any suggestion of compulsion either by the actions or words of the physician or others may be no consent at all and therefore may be successfully repudiated. In this context physicians must keep clearly in mind there may be circumstances when the initiative to consult a physician was not the patient’s but was rather that of a third party, a friend, an employer, or even a police officer.
“Under such circumstances, the physician may be well aware that the paitent is only very reluctantly following the course of action suggested or insisted upon by a third person. Then, physicians should be more than usually careful to assure themselves that patients are in full agreement with what has been suggested, that there has been no coercion and that the will of other persons has not been imposed on the patient”.
It is your body and it is your choice. You always have the right to do what’s best for you. True, empowered health cannot come from a place of coercion or pressure.
Know that you always have a choice–your doctor has a duty to inform you of your choice, as well as the information necessary for you to make the right choice for you, regardless of what is happening in the media or in politics.
Imagine that you’re stuck in the middle of the Amazon forest. You have no idea where you are. You’re terrified and hungry.
All of a sudden a man (or a woman) emerges from the bushes. They tell you, “I can help you get out of here. I can help you find your way home”. With relief, you follow them.
They slash through the bush with a certain confidence. They feel comfortable to be around. But after some time, doubt fills your mind.
A little while later you, still following this guide, but mind racing with doubt, both come upon someone else, coming from the other direction.
“That’s not the way out,” this new person exclaims, once you’ve greeted one another, “Follow me, I know how to get you out of here.” And there’s something about their scent or voice, you’re not sure what, but you like them better than the other guide, or maybe the same, you don’t know, but for whatever reason you choose to follow them.
And so you leave the first guide, thank them for their help (they really were helpful after all, but this new guide, well they’re really something) and all, and say, “My heart says I should follow this new guide”. And now you’re off, travelling in an entirely different direction, on what you hope is your way out of the jungle.
The truth is, every way is the way out. Perhaps some ways are faster than others, but one thing is certain, if you continue to travel in any one direction for a long enough period of time, you will eventually leave the dark woods.
What will keep you in the jungle, however, is switching direction, switching guides. Imagine you’re almost out of there: a few hundred metres away, and you find a new guide, turn around and immediately follow them further into the bush.
So it is with healing.
Sometimes we need to pick someone–a therapist, doctor, teacher, mentor, sometimes for no better reason than we like their voice or their website or we resonate with something they’re sharing from the heart–and we need to choose them and let them guide us.
No, we don’t need to do everything they say. We don’t need to follow them blindly. We can follow them with a sense of integrity and skepticism, of course, but if we choose their guidance, and their path towards healing, perhaps we need to see it through.
I find that, as it’s often the case with anxious patients, we constantly feel the need to reach for the new solution, the new single ingredient that will make us healthy and whole. That extra thing. That missing thing. That shiny new theory, or condition, or treatment.
“Perhaps I have histamine intolerance”
“Maybe I’m eating too many lectins”
“I think I need to test my oxalates”
“Maybe I’m zinc deficient”
“Maybe it’s my estrogen dominance”
It could be any one of those things, but if you find your wheels spinning, flipping from one therapist to another, and preventing any one of them from really getting a sense of who you are or what you need then I suggest you… stay.
Who do you stay with?
Stay with the one who listens.
If anyone is offering you a simple solution, a one-trick fix (and if any one is a one-trick pony, you know them, the ones who apply their theory to everyone they work with), then please run.
Your health and wellness does not boil down to one thing, one practice, one supplement, one root cause.
Stay with the one who listens. The one who repeats back to you what you said and adds more to it. The one who synthesizes and summarizes your problem in a way that clicks something into place.
Stay with the one who talks to you, not their team of followers.
The one who has your case information, not the yoga instructor you chat with after class while you’re putting your shoes back on, not the supplements salesperson who said “It’s probably your hormones” and hands you a bottle of 15 ingredients, not the documentary you watched on Netflix that applies one-size-fits-all diet advice to you and 6 billion others without even knowing your name.
Or, maybe stick with them… but stick with one of them. See their advice through to the end.
Maybe stick with the one who says, “Hm, this sounds like…” and proceeds to connect the dots for you, in front of your eyes. Who seeks to educate you. Who thinks about your case between visits. Who says things like “I consulted with my colleagues about your case to ask and…” and things like “I was thinking about/reviewing your case the other day and thought about…”
Stay with the one who refers you to other practitioners. Stay with the one who answers your pointed health questions with “It depends” or “Normally yes, but in your case…” or “A lot of the time no, but it’s possible that in your case…”
Psychoanalyst Francis Weller urges us to practice restraint. To pause. To reflect on our needs. He urges us to practice humility.
I love working with patients who show up humble, kneeling at the alter of their own healing, saying, “I found your website” or “My friend referred you” and then proceed to tell their stories, and receive my assessment.
They help me practice humility as well. To receive their cases with humility (not with my already always listening). To receive them with patience. To take my time. To do my research. To check in: “How does this sound…”.
I kneel at the alter of healing beside them.
We set an intention of working together–walking together—out of this wilderness.
I’m tired of hearing mental health conditions blamed on a “chemical imbalance”. Patients everywhere are being told that their mental health conditions are, literally, “all in their heads”. With this diagnosis—often distributed insensitively, and without much attention to the complex factors in thoughts, beliefs, emotions, the environment, biology, nutritional status, mental and emotional as well as physical stressors, and life circumstances (just to name a few) that can contribute to mental health imbalances—patients are left with the message that they are somehow damaged, broken, or that their condition arose out of an inherent weakness that they somehow possess. Through the numerous conversations I’ve had with those struggling with mental health symptoms, I have come to understand that oftentimes there are phrases that rob power more than the term “brain/chemical imbalance”.
Fortunately, there is still more to emerge in the wonderful world of science. Very little actual evidence supports the chemical imbalance theory of depression and researchers and clinicians alike are forced to admit that symptoms of conditions such as depression and anxiety are often the result of multiple factors that come together. Contrary to the common narrative of mental illness being a sign of weakness, evolutionary biologists are uncovering evidence that symptoms of depression might be the result of a highly adaptive strength based on preserving the body during times of great mental, emotional and physiological stress—showing, in fact, that depression and anxiety might in fact be afflictions of the strong, not the weak.
In my practice, I approach depression and anxiety from a functional medicine standpoint. This means, simply, that I look not at the title of the condition my patients come in with (I care very little if you have depression, or anxiety, or bipolar disorder, etc.—the name is not the thing itself), but how the condition occurs uniquely for them. By paying close attention to the multitude of symptoms, thoughts, and factors that influence the mood and emotions, I am able to uncover underlying pathways that point to imbalance in the body and dig up the roots from where the symptoms might have arisen in the first place. Through this method, focussing on the functioning of the body rather than it’s pathology, we’re able to bring the body back into a state of balance and reverse symptoms permanently, rather than simply slapping a band-aid over them.
When it comes to mental health, it is important to emphasize that depression and anxiety (as well as other mental health diagnoses) are not diseases at all; they are symptoms. When presented with low mood, feelings of sadness and worthlessness, lack of motivation, lethargy, brain fog, changes in appetite and weight, abysmal self-esteem and so on—all symptoms that many patients with depression face—we need to follow the threads of symptoms back to the point where things began unraveling. It is necessary to backtrack to the biological imbalances where symptoms first began.
There is an overwhelming amount of research coming out in the field of mental health that links the gut and digestive health to mental health symptoms, indicating that depression might not be a brain chemical imbalance at all, but a gut chemical imbalance. Where there is depression and anxiety, there is more often than not, a digestive issue.
We have always known that the digestive track and brain have an intimate bond. From the vagus nerve that enervates the gut and begins in the cranium, to the mood-regulating neurotransmitters that are created in the gut, we all have the experienced the tummy aches linked to grief or the power of anxiety to loosen our bowels. We’ve all noted the phenomenon that great ideas or moments of clarity seem to spontaneously arise from, not the brain, where we always assumed our thoughts were formed, but the gut (hence the term, “gut feeling”, which we use to characterize intuitive insights).
When it comes to issues with the brain—thoughts, moods, emotions, feelings, etc., where else should we look for answers than our brain’s close cousin, friend and confidant, the gut. Mental health symptoms can arise from impaired digestion in a number of ways:
A failure of the gut cells (enterocytes) to create neurotransmitters. The majority of serotonin (the “Happy Hormone”) is produced in the gut. Inflamed and unhappy gut cells are often unable to make serotonin.
An imbalance in the healthy gut bacteria that influences whole-body health. We have 10x more cells in our gut than in our body in the form of almost 5 lbs of symbiotic gut bacteria. This bacteria ensures our well-being by helping us digest our food, soothing inflammation, educating our immune system, killing off harmful pathogens, creating bulk for our stools and, relevant to the field of mental health, producing neurotransmitters important for regulating mood, such as serotonin and dopamine.
Research has gone into the connection between a low-level of inflammation in the brain and its affect on mood. Inflammation is usually a product of our diet, stress and food sensitivities. In naturopathic medicine and functional medicine we treat inflammation with the assumption that nearly all inflammation begins in the gut. A condition called “Leaky Gut” is a failure of the important seal between the intestinal walls and the rest of the body. When this seal is broken, toxins, proteins and other debris are free to enter the bloodstream, wrecking havoc, setting the immune system off course and, eventually, triggering symptoms of inflammation, autoimmunity and mental health issues.
Our body requires many building blocks to maintain its complex fortress. Difficulties in the digestive cells’ ability to absorb essential fats, amino acids and vitamins required for brain health, hormone regulation, detoxification and immunity, among the thousands of other chemical reactions in the body, will result in impairment in overall functional. Nutrient deficiencies are more common, even in developed societies, than one might think. Deficiencies arise from: impaired absorption, inadequate diet, increased amounts of stress and the ingestion of foods or medications the deplete the body of nutrients. In any case, optimizing the gut’s ability to digest and absorb the nutrients we’re either eating or supplementing is key for improving health and mood.
When it comes to understanding mental health issues I, as a clinician, realize it is hardly ever just one factor involved. Properly helping someone with anxiety or depression heal involves understanding the constellation of potential causes and how they inter-connect and relate to one another. Through this detective work, we can begin the journey of unraveling the imbalances and restoring the body’s ability to function and heal.
Treatment plans usually involve a combination of replenishing essential nutrients that patients are deficient in (deficiency can be detected through blood work, health history or symptoms), repairing the gut’s ability to absorb, restoring the body’s balance of healthy gut bacteria, removing food sensitivities and healing digestive inflammation, balancing hormones, and managing lifestyle stress and environmental factors that may be contributing to low mood.
My patients make impressive commitments to healing and are willing to examine their bodies and past experiences, in order to do the hard work of healing. Beyond my role as a doctor, I am committed to working as a facilitator, teacher and guide. My job is not to tell people the right path to walk, but to help them understand their body’s complex language, listen to the signals and messages that arise from it, and understand what those signals are asking of them.
For more information, click here. I run a practice with a special focus in mental health, youth mental health and hormonal conditions. I work in Bloor West Village in Toronto, Canada.
When our minds are stressed, how do our bodies react? We experience something called “adrenal fatigue” that can closely mimic the symptoms of depression.
Hi, naturopathic doctor, Talia Marcheggiani, here. I’m a mental health expert and I’m at Bloor West Wellness Clinic and today we’re going to talk about the Stress-Depression Connection.
Most of us are stressed in North America. There’s a major stress epidemic. We know that anywhere from 70-90% of doctors’ visits are directly or indirectly attributed to stress and the symptoms that it causes in the body.
Most people are stressed, I think the estimate is 70% to 90% of North American women are experiencing some kind of chronic stress. Many are unaware of it and very few are doing anything about it or actively managing their stress through methods of self-care, relaxation techniques, and other therapies to lower the cortisol, or the stress hormones, that are producing that chronic stress in the body.
So, physiologically, when we get stressed, so, let’s say, you know, you’re in the paleolithic times, you’re walking through the forest and you encounter a giant bear running towards you. Our bodies would immediately start secreting epinephrine, or adrenaline, which is the first stress hormone. This is released from the adrenal glands, these pyramid-shaped endocrine or hormone glands, located on top of both of our kidneys. Epinephrine, or adrenaline, many of us have felt the effects of before, this makes our heart race, we start sweating, we start to, you know, you might feel like you have to go to the washroom, you might notice digestive effects. What will happen is, our blood vessels will dilate, our pupils will dilate, so that we can’t see fine detail but we can see movement much more easily so we can see the subtle movements of the bear lunging towards us and our body is primed for fight, flight or freezing so that we can get away from this immediate stressor, this threat to our safety and survival.
And really incredible things can happen when we’re in this hyper-arousal state, this sympathetic nervous system state.
A friend of mine was walking in Greece and she fell off a side walk, the side walk just ended, and in the fall, she fell off like cliff, and one of her arms broke so, she managed, in this superhuman ability, that all of a sudden she had, through the adrenaline that was coursing through her body to deal with this stress and surprise, she with the hand that wasn’t broken, grabbed the edge of the sidewalk and pulled herself to safety. And this was a woman, my friend, that can’t even do one pull-up she can’t do pushups, she doesn’t have the arm strength to, in a calm and not hyper-aroused state, perform that kind of physical act.
So, epinephrine and the stress response is amazingly powerful. This stress response can save our lives if called into action for the right reasons and at the right time.
However what’s going on in North America now, is that, especially in this modern society that we live in, with technology and all of the stressors that we’re encountering on a day-to-day basis and the pressures we put on ourselves, we’re in the hyper-arousal state far more often than normal.
Back when we were chased by bears and we had to respond physiologically to that stressor, we would have just, as soon as we reached safety or finished fighting the bear, or froze, played dead, so the bear would walk away, we would have returned back to a state of relaxation. I mean, our hearts would have continued to pound as we kind of got over that stressor, but eventually we would have returned to our rest and digest state, our parasympathetic state.
Back in those days we used to work an estimated 15 hours a week hunting, gathering food, um, in our paleolithic time, in our hunter-gatherer times, which is what our genes have evolved to succeed in—our genes haven’t evolved to catch up with the rapid change in the environment that we’ve created for ourselves and so we’re not used to working 40 to 80-hour work weeks and racing home, through traffic, to pick up the kids and do after school activities and finish up late assignments, getting to get after 12 pm and getting up at 6 am to do a workout so we can lose weight and all of the things that are filling our lives and causing us stress.
The issue with many of the women that I work with, many of the people that I work with, is that we don’t really notice that we’re under stress, like a lot of people will say that they don’t feel stressed and then the signs and symptoms that they’re bodies are exhibiting point me in a direction of some kind of stress response.
So, I described what adrenaline/epinephrine do. But our body doesn’t have a very big reserve of adrenaline and epinephrine, so when we’re in that fight or flight response for prolonged periods of time, the adrenal glands, those pyramid-shaped glands on top of the kidneys, they start to secrete another hormone, called cortisol.
Cortisol has some similar effects, but it’s better for prolonged periods of stress. Cortisol kind of makes us feel alert, it gives us this grounded energy so we can be effective when we have these daily things thrown at us. So, when we wake up in the morning, we feel kind of groggy and then we start to feel alert, maybe we have a quick workout or cold shower or we eat something, we start to feel like we’re becoming alive, we’re greeting the day. That’s cortisol starting to build up in our bodies and prepare us for the things that we have to do, for the mental tasks, or the physical tasks, or the juggling of all the tasks that we have coming up for us in that day.
Cortisol is a good thing. We want to have cortisol because without it, we can’t perform, we can’t be who we need to be. And we can’t bring ourselves into the world and do the things that we’re supposed to do that day.
The problem is, of course, and I’ve already mentioned this, is when stress is prolonged and when stress is taking over more than 50% of our day and our bodies are in that fight or flight state for more time than they’re in the rest and digest state.
Some of the effects of being in this state and, as I mentioned, a fair amount of us are this state most of the time, or have to be. Some of the effects are high blood pressure, high cholesterol, heart diseases, even some cancers, suppressed immunity, things like skin issues, hormonal imbalances, such as infertility, or PCOS or endometriosis, changes in eyesight, changes in hearing, hair loss, acne, impotence, and various other symptoms. And, of course, depression and mental illness.
One of the effects of cortisol is that it can lower serotonin, which is the feel-good, the happy neurotransmitters that our brain secretes and dopamine, another neurotransmitter that promotes feelings of well-bring and happy mood and also helps with that motivation and reward cycle.
Cortisol also controls inflammation and, when we have too much of it, it suppresses inflammation, but once we start to become deficient in cortisol, inflammation can increase and when our body’s relying on cortisol all the time, the balance of cortisol can get thrown off and we can have highs and lows of cortisol in the body.
We know that there is an implication in inflammation and mood, so cortisol is often at the root of excess inflammation or inflammatory symptoms.
There’s also a condition that’s not really recognized in conventional medicine, but naturopathic doctors recognize, as well as functional doctors. So functional doctors and naturopathic doctors, we don’t really work with diseases that you come in with, I mean we work with those too, but where we really excel is when we’re looking at the patterns and the symptoms and the blood work showing disease processes before they actually become diseases. And I think depression and most mental health conditions fall in that area because we know that there’s no blood tests for things like depression. Direct blood tests, I mean. There’s no real diagnostic criteria beyond the subjective criteria that’s in the DSM V. So, when somebody’s depressed, we have to rely on a variety of symptoms and then I can order some blood tests to rule out why someone might be feeling that, but it’s not a disease like diabetes where you run lab tests and you can infer from those lab tests directly what’s going on in the person’s blood and in their body and in their cells. And, of course, the result or the solution for depression is much different than diabetes, especially type I diabetes where it’s an insulin deficiency, you inject insulin and the disease is managed.
With things like depression, we have to reason backwards and try and understand what might have led to those symptoms or what’s going on in the person’s body that’s causing this imbalance that’s causing the symptoms to arise.
So, back to adrenal fatigue. So, when patients come in, and they’re experiencing prolonged stress that begin with something called the resistance phase. So this is when you’re feeling like life is busy you have a lot on your plate, but it almost, you almost thrive in this situation. It feels kind of good. You feel like you’re in control, you feel motivated and you feel like you’re getting things done. You might be tired at the end of the day, you might not be sleeping as well as you could. And you’re definitely not feeling zen. You’re not feeling relaxed and like a Buddhist monk most of the time. You’re feeling that there’s pressure on you, but you’re coping. Things are ok. This is called the Resistance Phase. And this means that your body is producing enough cortisol to deal with the daily tasks at hand.
After months to years of this, however, if this prolonged and we’re not taking enough breaks to allow our bodies to replenish, we can experience something called Adrenal Fatigue. This is when our body’s not able to produce the cortisol needed to cover those daily tasks. So remember how I said that cortisol kind of makes us feel alert and alive and ready to deal with the day ahead of us. In Adrenal Fatigue we’re not able to activate that stress response when we need it because we’ve had it turned on all the time. It’s almost like the gas tank’s empty and we’re kind of sputtering to get it going again. We’re trying to get our car to run on the fumes that are leftover. And, we might call this Burnout, this is another word for it, is burnout.
And so, in adrenal fatigue, and this is a really common situation that often leads to depression and also often has symptoms that actually mirror or overlap with depression. In adrenal fatigue, first of all, the main symptom is just feeling tired, fatigued. There are sleep disturbances. We feel weak, we feel unmotivated, and one of the key symptoms is that we’re not relieved by exercise.
So a lot of my patients will tell me, “I want to exercise, I know I should exercise but I just don’t have the energy to exercise.” And I’ll ask them, “do you feel like you are able to push yourself to do some exercise, like go for a brisk 30-minute walk or even, you know, a quick jog. How do you feel afterwards?” And if they tell me they feel like it depletes them more, this is often a sign that they’re in that burnout phase, they’re in adrenal fatigue.
Because when you’re in a resistance phase, exercise can kind of boost your cortisol a little bit, so if you’re still able to make it, it feels pretty good because it kind of revives you and it perks you back up. But if you’re in an adrenal fatigue situation, you just don’t have the cortisol reserves to get through that exercise, to get through that workout and to feel good afterwards. So that’s one of the symptoms.
How cortisol is supposed to work in a healthy person that has adrenal glands that aren’t depleted, is when you wake up in the morning, your cortisol begins and it’s high. And that’s why you test blood and salivary cortisol in the morning as soon as you get up. So that means you wake up and you feel like you’ve slept pretty well and you’re ready to start the day, you feel alert. You’re not groggy, you don’t wish that you could just stay in bed for the rest of the day.
Throughout the day your cortisol will gradually decline. It might have a few dips and usually perks up with eating or exercise. So if you have a protein-rich, or carbohydrate-rich meal, your cortisol can come back up and that’s around meal-times you’ll feel a little bit more alert. And your cortisol will decline until bedtime when you feel tired and you feel ready to go to sleep and it will stay low throughout the night so you won’t be waking up at night. You’ll feel rested and if you have one of those sleep trackers or a Fitbit, it will show you that you have restful sleep and that you spend a lot of your time in REM sleep or deep wave sleep. And then the cycle starts again, you wake up, your cortisol starts to peak and gets higher again.
When our cortisol cycle is off. When we’re in adrenal fatigue or even the end stages of stress resistance, which proceeds that burnout adrenal fatigue stage and often proceeds depression. The resistance phase is more associated with anxiety, burnout is more associated with depression.
When we’re in that burnout phase, we’re not able to get the cortisol up in the morning so you wake up feeling exhausted. You will often even have a crash, you might kind of get going and ready to go or you might just be used to having that level of energy, on a scale of 1 to 10, you might be anywhere from a 3 to a 7. Around 10 am, though, you’ll notice a dip in your energy, so a lot of people will have this kind of energy crash around 10 am and then they get a second wind, they can kind of go. A very typical thing that happens is around 3-4 pm, 2-4pm, after lunch, there’s a massive energy crash and we’re still at work, most of the time, those of us that work 9-5 and so you’re at work and you’re just feeling exhausted.
And then people kind of get a second wind and another thing that happens, which is not great, is that you get a second wind right before bedtime. When you’re supposed to be going to sleep, you feel this kind of “tired and wired”, like you’re not able to, you know, wind yourself down to get a restful night’s sleep. You feel like you need to be up and on your electronics and doing some work, catching up on some things that you need to get done.
And eventually you might go to bed and usually this happens close to midnight or after midnight, and then most people will have a cortisol spike in the middle of the night between 2 and 4 am where you wake up and are unable to fall back asleep. And thus the cycle begins again where you had a spike in the middle of the night, your sleep’s been broken, you’re tired again in the next morning.
So how do we get out of this cycle? Because, you know, depression has low mood, depression has low motivation, depression has changes in weight and metabolism and appetite and these feelings of sadness and adrenal fatigue and burnout have a lot of those same symptoms. There’s not motivation, you’re gaining weight in the abdomen, you’re immune system is thrown off, you’re feeling just this general malaise and muscle pain and exhaustion and sadness and low mood and low self-worth and all of these things that we see in depression.
So how do we solve this? So the first thing we do is, if possible, we try and manage stress, to establish self care routines and this is a process that we need to work towards, it doesn’t happen in one visit, in a day it takes a few months to a few years to rebuild and reestablish. We make sure that we’re living a balanced life and we’re managing our cortisol and we also might prescribe supplements and herbs to stimulate cortisol production and to help our bodies manage stress and to help our adrenal glands work more optimally. And this often has a dramatic shift in mood after a few months. I have personal experience with this myself and it’s amazing. In a few months you look back to where you were and you notice big shifts.
It’s also necessary to make sure that blood sugar is not spiking throughout the day because cortisol and blood sugar are tightly interconnected. If our blood sugar drops, our body needs to create cortisol to bring it back up and likewise, if our blood sugar is high, this is a stress on the body and it can affect the cortisol balance. If our blood sugar is nice and steady and we’re eating enough fats and proteins to keep our neurotransmitters and our hormones productive and in production in the body, we notice a more even mood and energy level and this is really important so I go over nutrition and how to plan meals, especially in the morning with a protein and fat-rich breakfast.
And, finally, things like bodywork and things like, if not psychotherapy, then things to help with the life stressors that are going on, directly addressing those things. Even helping with the body stress response, the body’s perceived response because a lot of the time we have stress stored in our thoughts and emotions in the head, which is what addressed usually with many forms of psychotherapy. But oftentimes we also store stress in the body and so I find that acupuncture can be really affective and there’s studies that show that acupuncture actually outperforms Prozac in some 6-week trials as well as acupuncture can also help the brain move into that parasympathetic rest and digest state.
So, from 4-6 sessions of acupuncture can really shift us into a more relaxed state and help us with that stress response that we often be stuck in.
So, for more information, visit my website. I’m at TaliaND.com, or you can send me an email at connect@taliand.com. I work at Bloor West Wellness in Toronto. And if you want, leave your questions or comments below and we’ll start the discussion. Thanks, bye! 🙂
People seek out naturopathic doctors for expert advice. This immediately positions us as experts in the context of the therapeutic relationship, establishing a power imbalance right from the first encounter. If left unchecked, this power imbalance will result in the knowledge and experience of the practitioner being preferred to the knowledge, experience, skills and values of the people who seek naturopathic care.
The implicit expectation of the therapeutic relationship is that it’s up to the doctor to figure out what is “wrong” with the body patients inhabit and make expert recommendations to correct this wrong-ness. After that, it’s up to the patients to follow the recommendations in order to heal. If there is a failure to follow recommendations, it is the patient who has failed to “comply” with treatment. This “failure” results in breakdown of communication, loss of personal agency on the part of the patient, and frustration for both parties.
When speaking of previous experience with naturopathic medicine, patients often express frustration at unrealistic, expensive and time-consuming treatment plans that don’t honour their values and lifestyles. Oftentimes patients express fear at prescriptions that they had no part in creating, blaming them for adverse reactions, or negative turns in health outcomes. It’s common that, rather than address these issues with the practitioner, patients take for granted that the treatment plan offered is the only one available and, for a variety of reasons, choose to discontinue care.
One of the elements of Narrative Therapy—a style of psychotherapy founded by Australian Michael White—I most resonate with is the idea of the “therapeutic posture”. In narrative therapy, the therapist or practitioner assumes a de-centred, but influential posture in the visit. This can be roughly translated as reducing practitioner expertise to that of a guide or facilitator, while keeping the agency, decision-making, expertise and wisdom of the patient as the dominant source for informing clinical decisions. The de-centred clinician guides the patient through questioning, helping to reframe his or her identity by flushing out his or her ideas and values through open-ended questions. However, the interests of the doctor are set aside in the visit.
From the place of de-centred facilitation, no part of the history is assumed without first asking questions, and outcomes are not pursued without requesting patient input. De-centring eschews advice-giving, praise, judgement and applying a normalizing or pathologizing gaze to the patient’s concerns. De-centring the naturopathic practitioner puts the patient’s experiences above professional training, knowledge or expertise. We are often told in naturopathic medical school that patients are the experts on their own bodies. A de-centred therapeutic gaze acknowledges this and uses it to optimize the clinical encounter.
I personally find that in psychotherapy, the applicability of de-centring posture seems feasible—patients expect that the therapist will simply act as a mirror rather than doling out advice. However, in clinical practice, privileging the skills, knowledge and expertise of the patient over those of the doctor seems trickier—after all, people come for answers. At the end of naturopathic clinical encounters, I always find myself reaching for a prescription pad and quickly laying out out my recommendations.
There is an expected power imbalance in doctor-patient relationships that is taught and enforced by medical training. The physician or medical student, under the direction of his or her supervisor, asks questions and compiles a document of notes—the clinical chart. The patient often has little idea of what is being recorded, whether these notes are in their own words, or even if they are an accurate interpretation of what the patient has intended to convey—The Seinfeld episode where Elaine is deemed a “difficult patient” comes to mind when I think of the impact of medical records on people’s lives. After that we make an assessment and prescription by a process that, in many ways, remains invisible to the patient.
De-centred practice involves acknowledging the power differential between practitioner and patient and bringing it to the forefront of the therapeutic interaction.
The ways that this are done must be applied creatively and conscientiously, wherever a power imbalance can be detected. For me this starts with acknowledging payment—I really appreciate it when my patients openly tell me that they struggle to afford me. There may not be something I can do about this, but if I don’t know the reason for my patient falling off the radar or frequently cancelling when their appointment time draws near, there is certainly nothing I can do to address the issue of cost and finances. Rather than being a problem separate from our relationship, it becomes internal the the naturopathic consultation, which means that solutions can be reached by acts of collaboration, drawing on the strengths, knowledge and experience of both of us.
In a similar vein, addressing the intersection of personal finance and real estate within the therapeutic relationship requires a delicate balance of empathy and practicality. Patients may be navigating the complexities of homeownership or rental expenses, which can significantly impact their overall well-being. Encouraging open communication about these financial stressors fosters an environment where solutions can be explored collaboratively. It’s essential to recognize that financial challenges are not isolated issues but are intricately woven into the fabric of a person’s life, influencing mental and emotional well-being.
For instance, a patient might express concerns about the financial strain associated with homeownership, prompting a discussion about alternative housing options or budgeting strategies. In this context, exploring unconventional opportunities, such as innovative approaches to real estate like eXp Realty, could naturally arise. Integrating discussions about progressive real estate models within the therapeutic dialogue allows for a holistic exploration of solutions, leveraging the expertise and experiences of both the practitioner and the patient. This approach not only addresses immediate concerns but also lays the foundation for a collaborative and conscientious partnership in navigating the multifaceted aspects of personal finance and real estate.
De-centred practice involves practicing non-judgement and removing assumptions about the impact of certain conditions. A patient may smoke, self-harm or engage in addictive behaviours that appear counterproductive to healing. It’s always useful to ask them how they feel about these practices—these behaviours may be hidden life-lines keeping patients afloat, or gateways to stories of very “healthy” behaviours. They may be clues to hidden strengths. By applying a judgemental, correctional gaze to behaviours, we can drive a wedge in the trust and rapport between doctor and patient, and the potential to uncover and draw on these strengths for healing will be lost.
De-centred practice involves avoiding labelling our patients. A patient may not present with “Generalized Anxiety Disorder”, but “nervousness” or “uneasiness”, “a pinball machine in my chest” or, one of my favourites, a “black smog feeling”. It’s important to be mindful about adding a new or different labels and the impact this can have on power and identity. We often describe physiological phenomena in ways that many people haven’t heard before: estrogen dominance, adrenal fatigue, leaky gut syndrome, chronic inflammation. In our professional experience, these labels can provide relief for people who have suffered for years without knowing what’s off. Learning that something pathological is indeed happening in the body, that this thing has a name, isn’t merely a figment of the imagination and, better still, has a treatment (by way of having a name), can provide immense relief. However, others may feel that they are being trapped in a diagnosis. We’re praised for landing a “correct” diagnosis in medical school, as if finding the right word to slap our patients with validates our professional aptitude. However, being aware of the extent to which labels help or hinder our patients capacities for healing is important for establishing trust.
To be safe, it can help to simply ask, “So, you’ve been told you have ‘Social Anxiety’. What do you think of this label? Has it helped to add meaning to your experience? Is there anything else you’d like to call this thing that’s been going on with you?”
Avoiding labelling also includes holding back from using the other labels we may be tempted to apply such as “non-compliant”, “resistant”, “difficult”, or to group patients with the same condition into categories of behaviour and identity.
It is important to attempt to bring transparency to all parts of the therapeutic encounter, such as history-taking, physical exams, labs, charting, assessment and prescribing, whenever possible. I’ve heard of practitioners reading back to people what they have written in the chart, to make sure their recordings are accurate, and letting patients read their charts over to proofread them before they are signed. The significance of a file existing in the world about someone that they have never seen or had input into the creation of can be quite impactful, especially for those who have a rich medical history. One practitioner asks “What’s it like to carry this chart around all your life?” to new patients who present with phonebook-sized medical charts. She may also ask, “Of all the things written in here about you, what would you most like me to know?” This de-emphasizes the importance of expert communication and puts the patient’s history back under their own control.
Enrolling patients in their own treatment plan is essential for compliance and positive clinical outcomes. I believe that the extent to which a treatment plan can match a patient’s values, abilities, lifestyle and personal preferences dictates the success of that plan. Most people have some ideas about healthy living and natural health that they have acquired through self-study, consuming media, trial-and-error on their own bodies or consulting other healthcare professionals. Many people who seek a naturopathic doctor are not doing so for the first time and, in the majority of cases, the naturopathic doctor is not the first professional the patient may have consulted. This is also certainly not the first time that the person has taken steps toward healing—learning about those first few, or many, steps is a great way to begin an empowering and informed conversation about the patients’ healing journey before they met you. If visiting a naturopathic doctor is viewed as one more step of furthering self-care and self-healing, then the possibilities for collaboration become clearer. Many people who see me have been trying their own self-prescriptions for years and now finally “need some support” to help guide further action. Why not mobilize the patient’s past experiences, steps and actions that they’ve already taken to heal themselves? Patients are a wealth of skills, knowledge, values, experiences and beliefs that contribute to their ability to heal. The vast majority have had to call on these skills in the past and have rich histories of using these skills in self-healing that can be drawn upon for treatment success.
De-centring ourselves, at least by a few degrees, from the position of expertise, knowledge and power in the therapeutic relationship, if essential for allowing our patients to heal. A mentor once wrote to me, “Trust is everything. People trust you and then they use that trust to heal themselves.”
By lowering our status as experts, we increase the possibility to build this trust—not just our patients’ trust in our abilities as practitioners, but patients’ trust in their own skills, knowledge and abilities as self-healing entities. I believe that de-centring practitioner power can lead to increased “compliance”, more engagement in the therapeutic treatment, more opportunities for collaboration, communication and transparency. It can decrease the amount of people that discontinue care. I also believe that this takes off the burden of control and power off of ourselves—we aren’t solely responsible for having the answers—decreasing physician burnout. Through de-centring, patients and doctors work together to come up with a solution that suits both, becoming willing partners in creating treatment plans, engaging each other in healing and thereby increasing the trust patients have in their own bodies and those bodies’ abilities to heal.
Premature Ovarian Failure no longer bears that name. It’s not a failure anymore, but an insufficiency. POF becomes POI: Premature Ovarian Insufficiency, as insufficiency is apparently a softer term than “failure”. For me, it’s another telling example of how our society fears the names of things, and twists itself into knots of nomenclature and terminology rather than facing pain head-on. In this case, the pain is derived from the simple fact that the ovaries do not respond to hormones, that they for some reason die at an early age and cause menopause to arrive decades before it’s due, leading to infertility and risk of early osteoporosis.
Insufficiency, for me at least, fails to appease the sensitivity required for naming a problem. It reminds me of a three-tiered scoring system: exceeds expectations, meets expectations, insufficient performance. These reproductive cells have not been up to task. They’ve proven to be insufficient and, in the end, we’ve labelled them failures anyway—premature ovarian disappointments. Our disdain for the bodies we inhabit often becomes apparent in medical jargon.
What expectations do we have for our organs, really? For most of us that they’ll keep quiet while we drink, stay up late and eat what we like, not that they will protest, stop our periods, make us itch or remind us that we are physical beings that belong here, to this earth, that we can sputter and shut down and end up curb side while we wait for white coats to assist us. Our organs are not supposed to remind us of our fragile mortality. When it comes to expectations overall, I wonder how many of them we have a right to.
In one week I had two patients presenting with failures of sorts. With one it was her ovaries, in another it was his kidneys, first his left, now his right. Both of them were coming to me, perhaps years too late, for a style of medicine whose power lies mainly in prevention or in stopping the ball rolling down the hill before it gains momentum. When disease processes have reached their endpoint, when there is talk of transplant lists and freezing eggs, I wonder what more herbs can do.
And so, when organs fail, I fear that I will too.
In times of failure, we often lose hope. However, my patients who have booked appointments embody a hope I do not feel myself, a hope I slightly resent. In hope there is vulnerability, there is an implicit cry for help, a trust. These patients are paying me to “give them a second opinion”, they say, or a “second truth”.
I feel frustration bubble to the surface when I pore over the information I need to manage their cases. At the medical system: “why couldn’t they give these patients a straight answer? Why don’t we have more information to help them?” At my training: “Why did we never learn how to treat ovarian insufficiency?” At the patients themselves: “Why didn’t he come see me earlier, when his diabetes was first diagnosed?” And again at the system: “Why do doctors leave out so much of the story when it comes to prevention, to patient power, to the autonomy we all have over our bodies and their health?” And to society at large: “Why is naturopathic medicine a last resort? Why is it expensive? Why are we seen as a last hope, when all but the patients’ hope remains?”
Insufficiency, of course, means things aren’t enough.
I feel powerless.
There is information out there. I put together a convincing plan for my patient with kidney failure. It will take a lot of work on his part. What will get us there is a commitment to health. It may not save his kidneys but he’ll be all the better for it. My hope starts to grow as I empower myself with information, studies some benevolent scientists have done on vitamin D and medicinal mushrooms. Bless them and their foresight.
As my hope grows, his must have faded, because he fails to show for the appointment. I feel angry, sad and slightly abandoned—we were supposed to heal together. Feelings of failure are sticky, of course, and I wonder what story took hold of him. was it one that ended with, “this is too hard?” or “there is no use?” or “listen to the doctors whose white coats convey a certainty that looks good on them?”
A friend once told me, the earlier someone rejects you, the less it says about you. I know he’s never met me and it’s not personal, but I take it personally anyways, just as I took it personally to research his case, working with a healing relationship that, for me, had been established since I entered his name in my calendar. In some way, like his kidneys, I’ve failed him. Since we’re all body parts anyways, how does one begin to trust another if his own organs start to shut down inside of him? Why would the organs in my body serve him any better than the failing ones in his?
I get honest with my patient whose ovaries are deemed insufficient (insufficient for what? We don’t exactly know). I tell her there aren’t a lot of clear solutions, that most of us don’t know what to do–in the conventional world, the answer lies mainly in estrogen replacement and preserving bone health. I tell her I don’t know what will happen, but I trust our medicine. I trust the herbs, the homeopathics, nutrition and the body’s healing processes. I admit my insufficiency as a doctor is no less than that of her ovaries, but I am willing to give her my knowledge if she is willing to head down this path to healing with me. Who knows what we’ll find, I tell her, it might be nothing. It might be something else.
It takes a brave patient to accept an invitation like the one above; she was offered a red pill or a blue pill and took a teaspoon of herbal tincture instead. I commend her for that.
There aren’t guarantees in medicine but we all want the illusion that there are. We all want to participate in the game of white coats and stethoscopes and believe these people have a godlike power contained in books that allows them to hover instruments over our bodies and make things alright again. Physicians lean over exposed abdomens, percussing, hemming and hawing and give us labels we don’t understand. The power of their words is enough to condemn us to lives without children, or days spent hooked up to dialysis machines. We all play into this illusory game. They tell us pills are enough… until they aren’t. This is the biggest farce of all.
I can’t participate in this facade, but I don’t want to rob my patient of the opportunity for a miracle, either. We share a moment in the humility of my honesty and admission of uncertainty. I know my patients pay me to say, “I can fix it.” I can try, but to assert that without any degree of humility would be a lie. How can one possibly heal in the presence of inauthenticity? How can one attempt to work with bodies if they don’t respect the uncertain, the unknown and the mysterious truths they contain? In healing there is always a tension between grasping hope and giving in to trust and honestly confessing the vulnerability of, “I don’t know.”
For my patient I also request some testing—one thing about spending time on patients’ cases and being medically trained is that you get access to information and the language to understand it. I notice holes in the process that slapped her with this life-changing diagnosis.
When her labs come back, we find she might not have ovarian insufficiency after all. Doorways to hope open up and lead us to rooms full of questions. There are pieces of the story that don’t yet fit the lab results. I give her a list of more tests to get and she thanks me. I haven’t fixed her yet, but I’ve given her hope soil in which to flower. I’ve sent her on a path to more investigations, to more answers. And, thanks to more information in the tests, I’ve freed her and her ovaries from the label of “failure” and “insufficient” and realized that, as a doctor, I can free myself of those labels too. The trick is in admitting, as the lab results have done in their honest simplicity, what we don’t know.
For the moment, admitting insufficiency might prove to be sufficient in the end.
In most service industries, there are certain guarantees. If you go to a restaurant, your soup is guaranteed. At the GAP, you will get a pair of chinos, guaranteed. In lots of instances, you get what you are paying for and in most cases, you get to see if before you hand over your credit card—a coffee, a massage. In many cases, if you’re not satisfied, you can get your money back—guaranteed.
This is not the case in medicine. We cannot legally guarantee results. There are no guarantees.
Everybody and every body is different. Contrary to what it might seem like in our age of paralyzing fear of uncertainty, no one has all, or even most, of the answers.
Dr. Google makes it seem like we do, though.
When I see a new patient who is worried about their health and their future, I want to be able to promise them. I want nothing more than to say, “these breathing exercises will eliminate your anxiety, just like you asked for: poof! gone.”
I want to guarantee things.
I want to tell someone that, if they follow my instructions, they’ll never have another hypertensive emergency again. I want to, but I can’t. No one can. And our job is not to guarantee. It is to serve.
A $10,000 bag of chemotherapy pumped into your arm will not guarantee that the cancer goes into remission no matter how many studies show it has an effect. I can’t promise you’ll get pregnant, even though I’m doing my best, you’re doing your best and science is doing its best.
That’s all I can guarantee: that I will try my very best.
I can be your researcher, teasing out the useful scientific information from a sea of garbage and false promises—false guarantees from those who have no business guaranteeing anything. I can provide my knowledge, culminated from years of study and practice and life. I can sit with you while you cry and hear you share your story. I can let you go through your bag of supplements, bought in a whirlwind of desperation, and tell you what is actually happening in your body—something that doctor didn’t have time to explain. I have time to spend with you. We can have a real conversation about health. I can also make recommendations based on my clinical experience, research and millenia of healing practices. These recommendations will certainly help—virtually everyone sees some kind of benefit—but I can’t guarantee that either.
I watched a webinar on probiotics recently. The webinar sent me into a spiral of existential probiotic nothingness. I’ve been prescribing probiotics for years. I’ve seen benefits from them with my own eyes. Patients have reported great things after taking them and I feel better when I take them: my stomach gets flatter, things feel smoother, my mood gets lighter. Probiotics are wonderful. However, according to the research that was being presented by this professional, which he’d meticulously collected and organized, many things we thought about probiotics aren’t true. I’d have to change my whole approach when it came to probiotics, prescribing certain strains for certain conditions where they’d seen benefit. I remember feeling hard-done by by the supplement companies and the education I’d gotten at my school. How could we be so off base on this basic and common prescription?
At the same time, some skeptics were harassing me on Twitter, telling me that I’d wasted 4 years, that naturopathic medicine is useless and doesn’t help people. Besides having helped numerous people and having been healed myself, their words got to me. What if everything I know is as off-base as my previous knowledge on probiotics was?
The very next day, I called a patient to follow up with her. She’d kind of fallen off the radar for a while. She was happy to hear from me. I asked her how she was feeling, if she’d like to rebook. “I don’t need to rebook,” She told me, excitedly, “I’m completely better!”
After one appointment.
I was astounded and intrigued. Of course, we expect people to get better, but it takes time to heal, and I rarely go gung-ho on the first appointment, there was still lots left in my treatment plan for her. She’d been experiencing over seven years of digestive pain, debilitating fatigue, life-changing and waist-expanding cravings for sugar. It takes a while to reverse seven years of symptoms. It takes longer than a couple of weeks. But her symptoms were gone. She felt energized, her mood was great and she’d lost a bit of weight already. She no longer had cravings.
And she’d just started on one remedy.
Which was, you guess it, probiotics.
Sure, you might think. Maybe it wasn’t the probiotics, maybe she would have just gotten better on her own. Possible, but unlikely. She’d been suffering for years.
Ok, then, you say, maybe it was a placebo effect. Maybe it wasn’t the actual probiotics. Again, it’s possible. She’d tried other therapies before, which hadn’t worked, however and she “believed” in them just as much as the probiotic. And the probiotic made her better.
The point is this: we don’t know. Science is magical. People are magical. Medicine, which combines science with people, is the most magical of all. There are no guarantees.
The point is that anything can make anyone feel better: a good cry, a $10,000 bag of chemotherapy, journalling for 12 weeks or popping a probiotic. Some things have more research behind them. Some things we’ve studied and so we know some of the mechanisms for why things work. But we still have a lot of why’s and we always will. Everybody and every body is different. No two people or two conditions should receive the exact same protocol or supplement or IV bag or journalling exercise or cry-fest. We have no guarantees what will work or what will make you feel better. Just some research papers, some experience, maybe the odd dash of intuition or interpersonal connection and a firm resolve to want our patients to get better. And that’s a guarantee.
It seems like the only thing I can focus on right now is negative space.
Like the obsession with the space between a model’s waif-like thighs, affectionately termed the “thigh gap”, I have seemingly been attributing way too much time and attention to the lack of things in my life. Life is up in the air right now—a freeze-frame of dust particles that someone has stirred up, and we all wait breathlessly to see where they will settle on the ground.
That’s it: I feel unsettled.
And this unsettled feeling has the tendency to sharpen the focus on the things I don’t have in life. The search doesn’t need to go far. I lack stability in my career, a romantic relationship, my own apartment—the typical signs that life is moving forward. I don’t know what two months will bring, let alone the next few years and, as someone who spent all but two years of their waking adult life in academia, not having a future laid out before them in the form of assignments, tests and other externally imposed milestones leaves me feeling uncontained. There is no one conducting evaluations on my life but myself.
And what an astute evaluator I’ve become:
How am I doing? The best way for the masochist to answer this question is to look at how other people are doing. There are plentiful points of comparison if I want to feel fully inferior. Everyone seems to have more patients than I do, nicer apartments and fulfilling relationships. They seem to be moving somewhere. I just feel stuck, not at a crossroads, but at the edge of a cliff. Am I just supposed to jump? Did everyone else jump? Or did they end up hitching a ride on some lucky parachute that happened to pass by a few minutes before me? Why are they lucky? What are my eyes closed to? When will it be my turn? Or am I simply cursed? The mind stirs up more dust. Sense of personal injustices prevail.
This unsettled feeling can’t last.
So I strive. The answer must lie in working harder. After all, it’s what we’re told to do. Push on. Move forward. Just do it, as Nike says, sweat beading on foreheads. There’s always sweat beading on the foreheads of the mentally unsettled.
I hand out business cards, but no one calls me. I try calling them. I look for other jobs that are poor fits. I take more shifts at the day-job I’m holding on to for secure cash. I go to business networking meetings that I don’t connect with and try to convince myself that I should just force myself to make it work. I search desperately for an apartment, and despair when I don’t get the one I finally love. I hold on to past relationships well past their due dates and complain and obsess and analyze what went wrong to my friends, whose patience can’t possibly last much longer. I notice myself compromising my values and dreams in order to get away from the edge of the cliff.
Still I get nowhere.
So I turned to the only thing I know how to when the mind is desperate and despairing and the spirit is looking to the future for salvation—I turn to the present. The dust in up in the air, so to speak. Everything is unsettled. And yet, how am I? I’m more or less alright. I’m warm. I’m fed. I’m rested. My plight is ridiculous when compared to tiny Vietnamese hands sewing buttons on Banana Republic blouses. Who taught me this sense of entitlement?
I have a place to live and some money coming in (the longer it takes me to find an apartment, consequently, the more I end up saving). I have friends who are genuinely concerned about me and a generous, loving and supportive family. I have hobbies and social events to attend. The blessings in my life are numerous.
Why am I so intent on speeding down the highway of life? What will happen when I arrive at my destination? When I have a beautiful apartment, patients booked months in advance, when I’m in a wonderful, loving and passionate relationship with someone who inspires me, what will I do then? Once the dust is settled, won’t I eventually, decide to stir it up again? If I can’t be content in the present, when will I ever find that elusive contentment that always seems to slip out of our grasp?
Most of all, I ask myself, what is behind my longings? Are the reason I long for these things pure? Or, like a perfume or Coca-Cola ad, do I really want what’s behind what they’re selling me: the beauty, enchantment, lightness, freedom and magic that life often promises us but we seldom encounter in the places we’re told to look.
I wonder if, with eyes closed and mind settled, I’ll be able to breathe clear air again. Perhaps then I’ll find a path down from this cliff, a creative alternative to the already available options: jumping, backing down or sitting and waiting for a magical parachute to come and save me.
Between all the wants, needs, dreams and aspirations, between the striving is space. In that space I might find a little room to breathe. But who can really breathe with dust in their lungs?