We’ve been hearing quite a lot about The Science these days. So, what is science? How does science guide medical practice and naturopathic medicine?
The science council defines science as, “the pursuit and application of knowledge and understanding of the natural and social world following a systematic methodology based on evidence.” The answer is, science is a methodology.
It is applied in medicine through Evidence Based Medicine (EBM) which starts with the individual patient and incorporates: clinical expertise, scientific evidence (that best that exists according to a hierarchy), and patient values and preferences.
“Evidence medicine is the conscientious, explicit, judicious and reasonable use of modern, best evidence in making decisions about the care of individual patients. EBM integrates clinical experience and patient values with the best available research information.”
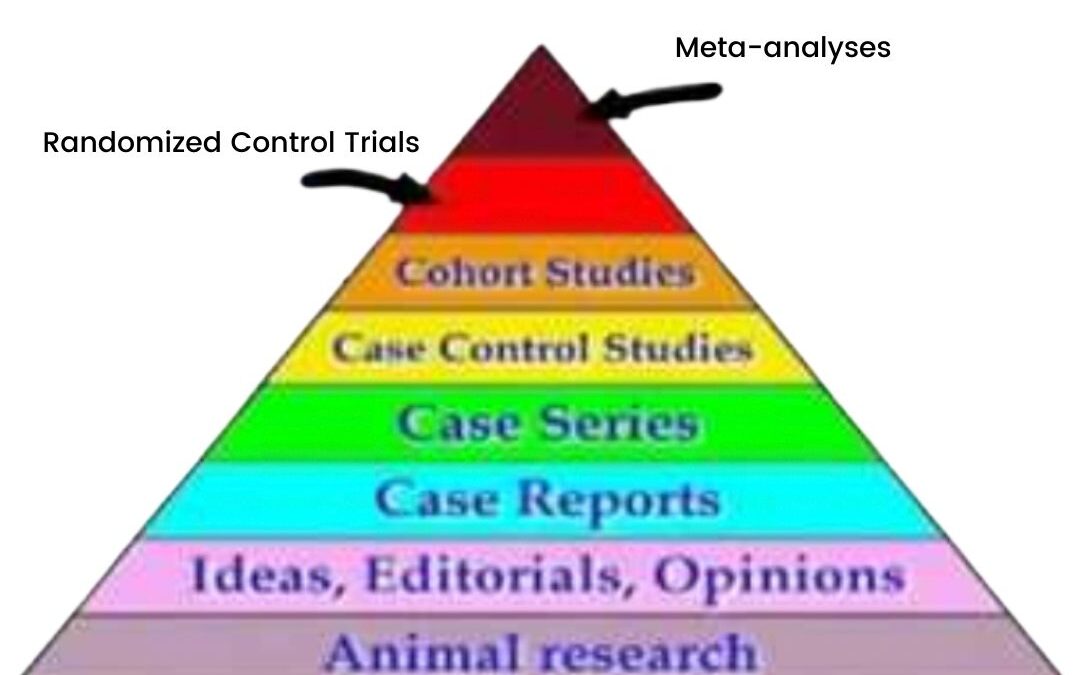
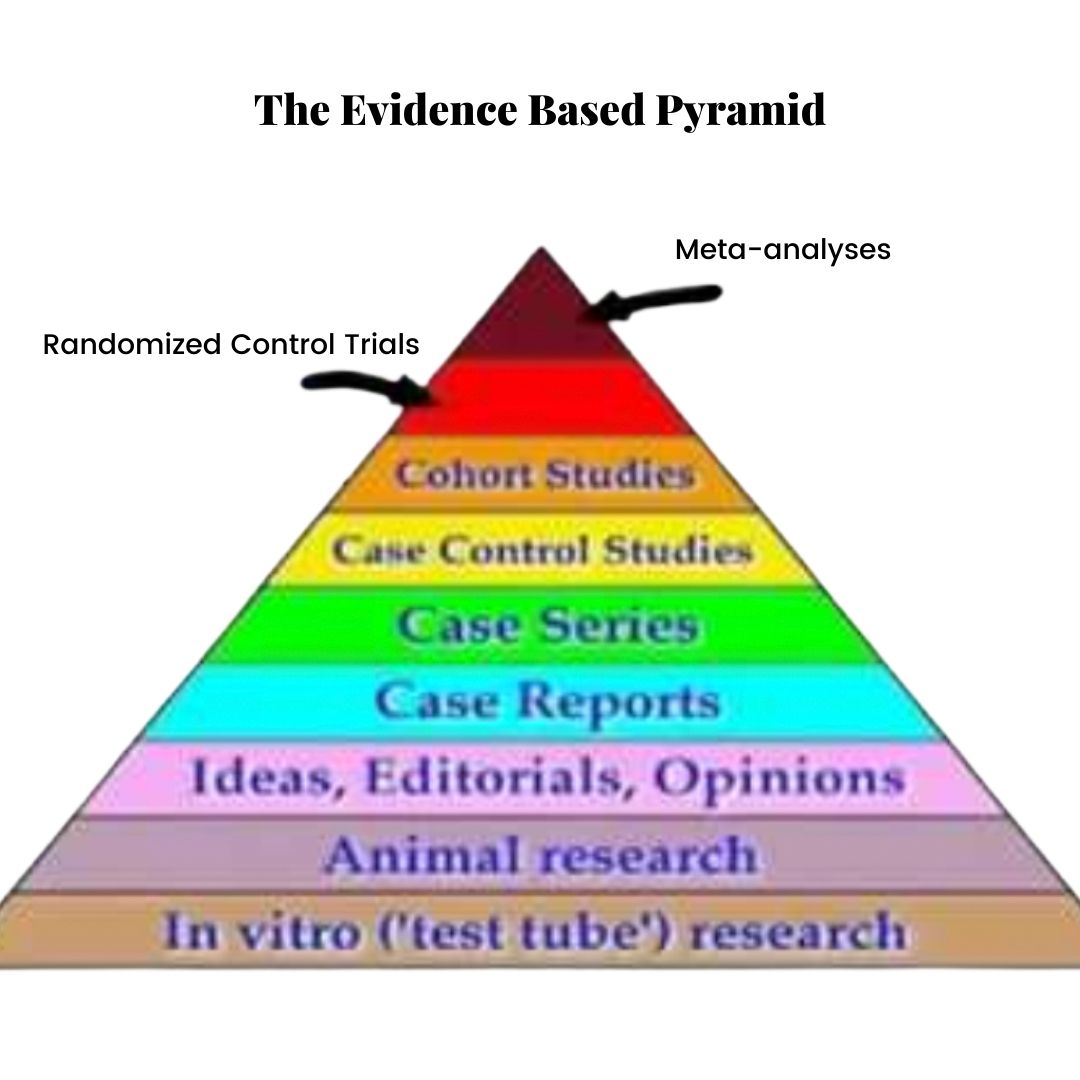
The Evidence-Based Pyramid
In EBM, evidence exists in a hierarchy, represented by the Evidence Based Pyramid (shown above). Animal studies are at the bottom, case reports (clinical anecdotes) somewhere in the middle and randomized control trials and meta-analyses (the Gold Standard of evidence) at the top.
Dave Sackett (the Father of EBM) et al. write in the British Medical Journal (1996),
“Good doctors use both individual clinical expertise and the best available external evidence and neither alone is enough.”
In addiction to scientific evidence, EBM must incorporate:
Patient values
A bottom-up approach (it is patient-centred, not guideline-centred)
The needs of the individual (EBM is not a one-size-fits-all formula)
Clinical expertise
The best available evidence: this does not mean using only randomized control trials. Sometimes the best evidence we have are case reports, historical and traditional use of an herb or animal studies. We still owe our patients the opportunity to see if a treatment works for them, especially if the risk of a given treatment is low.
As clinicians, we use our knowledge in different ways. We start with an assessment of the individual in front of us. This assessment takes into account the factors that influence this patient’s life, their lifestyle, their health condition and their overall health goals.
We then turn to clinical experience, research, our scientific knowledge and guidelines.
We share this information with our patient. Our job is to educate and convey the options so that the individual can provide informed consent. How does this knowledge fit into the patient’s life? How does it inform their choice?
Science is not a set of values. It is not a religion. We do not follow it.
Science provides us with a methodology for seeking the answers to questions we might ask about how the principles of nature, including the human body, are organized.
Science encourages us to ask questions and testing hypotheses in order to find answers.
It is never settled.
Most of all, science doesn’t tell us how to use scientific knowledge.
Our choices are governed by our goals, preferences and values.
So, “follow the sicence?”
No. Follow your goals, preferences, values and dreams.
And use science to help guide your way.
Reference:
Sackett, D. L., Rosenberg, W. C., Gray, J. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. BMJ, 312(7023), 71–72.
Brett Weinstein and Heather Heying have a t-shirt that says “Welcome to Complex Systems” on it.
Indeed.
Many patients and biological reductionism want to know what caused my anxiety, depression, hormonal issues, and autoimmune disease? What did I do wrong, or that went wrong for me? What was the food I failed to eat, the ingredient I was missing or the thing that caused the house of cards that represented my health to topple?
I think it’s appropriate to answer, “welcome to complex systems.”
Like everything else in nature, your body, your mental health is a complex system. This means that it consists of many factors, many of which have yet to be identified, virtually all that have yet to be correctly understood, that drive its function—even seeing health as an absence of disease, which is essentially how our medical system is organized, is a product of biological reductionism. Biological (or rather mechanical reductionism), the attempt to identify the loose screw or the spring that’s out of place, works for your car, but it doesn’t work for your brain, body, mental or physical health.
Understanding health might be better done using the Biopsychosocial Model, a framework for understanding where we sit today in terms of our health from the context of our biology, psychology, and social environment. Further, the biology part of the biopsychosocial factors that drive our health can be considered triggers and drivers rather than cause and effect.
Say you are feeling terrible. You’re feeling exhausted and agitated, and you’re constipated, and your hair is falling out. You see your doctor, and they tell you everything is great. You push for some bloodwork. Your doctor says your thyroid is slightly off, but it’s likely nothing.
So you take the bloodwork to your naturopathic doctor, who tells you your stimulating thyroid hormone, or TSH, is out of range, indicating that your thyroid seems to be under-functioning. They order more testing to understand what else lies under the hood and find your anti-thyroid antibodies are sky-high. It turns out you might have Hashimoto’s thyroiditis or a condition of under-functioning thyroid driven by autoimmunity.
You also have celiac and a family history of multiple sclerosis, thyroid issues, and other autoimmune diseases. How did this happen?
For months you were dealing with a ton of stress. You also haven’t been eating the greatest. But you haven’t been sleeping well either, and it’s hard to eat well when you’re so darn tired. You’ve been working a lot, dealing with a global pandemic and all, and things haven’t been great. But this is compounded by the fact that you’re not feeling great, which makes it harder to deal with the stress, making the condition worse–a vicious cycle.
At least now you know that something is going on, and it’s not all in your head, but what caused this?
We want to know the exact cause of something to find the specific treatment. This is biological reductionism. Something is missing; we’ve identified the thing, so here’s the magic bullet that will target the exact issue and either replace it or weed it out.
The problem with complex systems is that when we pull one thread on this ball of yarn that is your health, a knot gets tightened somewhere else. Like the post on Chesterton’s fence, complex systems are difficult to understand. So we must assume we don’t fully understand them, and therefore I believe we should exercise humility when it comes to tugging on pieces of yarn that comprise the whole operation.
For example, the side effects of drugs aren’t side effects; they’re effects. Some of these effects are wanted. But all the other effects that happen, such as weight gain, agitation, or migraines from anti-anxiety medication, are unwanted. And they are still effects of the drug. Side effects of drugs are indications that we have failed to understand the implications of messing with complex systems entirely.
Sometimes this might be warranted. The system might be so far out of bounds that it could kill you unless we intervene. Sometimes the drug is more specific–if you don’t have a thyroid, you need thyroid hormone. However, does the thyroid have a role beyond simply producing T4 (thyroid medication)? While thyroid hormone medication might be indicated or necessary, is it fully completing the thyroid’s function in the complex system? What about T3? (or T1 and T2)? What about iodine? What about the driver contributing to thyroid dysfunction? Is it still driving disease? Might it start to create other symptoms elsewhere in the body?
In other words, have we entirely dealt with the problem when we reduce thyroid dysfunction down to deficiency of a single hormone?
So, I explain to my patient; there isn’t a cause of autoimmune disease or a thyroid condition. There are drivers, such as chronic inflammation (which might be triggered by a specific food your immune system doesn’t like). There might be a driver like chronic stress triggered by a more stressful event. Genes can be drivers or susceptibilities triggered by environmental factors, such as nutrient deficiencies. So, it’s not gluten that caused your thyroid issue, but it might start or driveimmune system overactivation and chronic inflammation, contributing to the problem.
So what does this mean for treatment? It means we need to look at the ball of yarn respectfully. We need to appreciate how many symptoms are a healthy response and compensation by the body. If we randomly attack a symptom like fatigue with a stimulant, we might further drive the inflammation, nutrient deficiencies, or stress that underly that symptom. We need to understand what the body lacks (what’s it deficient in?) and when it might have too many environmental toxins, allergens, chronic stress, blue light, etc.
We need to look at the system and help it re-establish its equilibrium. Cleaning up garbage in a pond is likely a good idea–it probably shouldn’t be there in the first place. The pond didn’t create the trash. But what about something else we don’t want, like an algae overgrowth? But if we throw an algaecide in the water, what unseen harm might we be doing to the pond’s ecosystem if we mess with it? Has the pond created algae for the reason that currently escapes us, but wouldn’t if we looked a little deeper?
Why doesn’t our modern medical model treat our bodies as complex systems? I’m not sure. A few guesses, though. Complex systems are complicated, if not impossible, to understand. They require time to unravel. They need patience and education. They require effort on the part of the patient to try to shift their environment to eliminate or adjust possible triggers. They are impossibly hard to market and profit from.
Getting our concept of a complex system “right” can take time. It might take trial and error, collecting information, curiosity, and a willingness to try. It might take admitting that our culture has many aspects to it that are inherently unhealthy.
We might have to find a mini culture where people get sun, eat well, move, and sleep early to support our health. We might have to be “stricter” than the people around us. These people may have similar drivers working below the surface, but their symptoms may look different. They do not display symptoms like fatigue or anxiety until their systems have completely shifted beyond balance.
We are all a manifestation of complex systems. Laini Taylor says, “Inside each of us, there is a world that no one else can ever know or see or visit.”
“I don’t believe in diseases anymore, I treat stories.
“…No other medical system in the world ever believed in diseases. They all treat everybody as if, you know it’s whether it’s the ancestors or meridians–it’s none of this rheumatoid arthritis, strep throat kind of thing. That’s just this construct that we kind of… made up.”
– Dr. Thomas Cowan, MD
Dr. Cowan is admittedly a (deliciously) controversial figure. His statement, I’m sure, is controversial. But that’s why it intrigues me.
In naturopathic medicine, one of our core philosophies, with which I adhere very strongly, is “treat the person, not the disease”.
And, in the words of Sir William Osler, MD, “It is much more important to know what sort of person has a disease, than to know what sort of disease a person has”.
And, I guess it’s relevant to ask, what is disease in the first place?
I see disease as an non-hard end point, a state that our biological body enters into. On the continuum between perfect health (which may be an abstract and theoretical construct) and death, disease I believe is near the far end of the spectrum.
Disease happens when the body’s proteins, cells, tissues, or organs begin to malfunction in a way that threatens our survival and disrupts our ability to function in the world. For example, a collection of cells grows into a tumour, or the immune system attacks the pancreas and causes type I diabetes.
But, of course there is always more to the story.
What causes disease?
I have heard biological disease boiled down to two main causes: nutrient deficiencies and toxicities. And, I’m not sure how strongly I agree with this, but on a certain level I find this idea important to consider.
However, it is definitely not how Western Medicine views the cause of disease!
Diseases, as they are defined, seem to be biological (as opposed to mental or emotional). They have clinical signs and symptoms, certain blood test results, or imaging findings, and they can be observed looking at cells under a microscope.
Medical textbooks have lists of diseases. Medicine is largely about memorizing the characteristics of these diseases, differentiating one from another, diagnosing them, and prescribing the treatment for them.
As a naturopathic doctor, I see a myriad of patients who don’t have a “disease”, even though they feel awful and are having difficulty functioning. These patients seem to be moving along the disease spectrum, but their doctors are unable to diagnose them with anything concrete–they have not yet crossed the threshold between “feeling off” and “disease”.
Their blood tests are “normal” (supposedly), their imaging (x-rays, MRIs, ultrasounds, etc.) are negative or inconclusive, and their symptoms don’t point to any of the diseases in the medical school textbooks.
And yet they feel terrible.
And now they feel invalidated.
Often they are told, “You haven’t crossed the disease threshold yet, but once you reach the point where you’re feeling terrible and our tests pick it up too, come back and we’ll have a drug for you”.
Obviously not in so many words, but often that is the implication.
Our narrow paradigm of disease fails to account for true health.
Even the World Health Organization states that health is not the mere absence of disease.
So if someone does not have health (according to their own personal definition, values, dreams, goals, and responsibilities), but they don’t have disease, what do they have?
They have a story.
And I don’t mean that what they’re dealing with is psychological or mental or emotional instead, and that their issues are just “all in their head”. Many many times these imbalances are very biological, having a physical location in the body.
Subclinical hypothyroidism, insulin resistance, nutrient deficiencies, chronic HPA axis dysfunction, and intestinal dysbiosis are all examples of this. In these cases we can use physical testing, and physical signs to help us identify these patterns.
An aside: I believe the categories of biological, mental, environmental, and emotional, are false.
Can we have minds without biology? Can we have emotions without minds or physical bodies? How do we even interface with an environment out there if we don’t have a body or self in here?
Aren’t they all connected?
Ok, back to the flow of this piece:
Your story matters.
This is why it takes me 90 minutes to get started with a new patient.
It’s why I recommend symptom and lifestyle habit tracking: so that we can start to pay attention.
It’s why I’m curious and combine ancient philosophies, research (because yes, research is useful, there’s no doubt–we should be testing out our hypotheses), and my own intuition and skills for pattern-recognition, and my matching my felt-sense of what might be going on for a patient with their felt sense of what they feel is going on for them.
Attunement.
I write about stories a lot. And I don’t mean “story” in a woo way, like you talk about your problems and they go away.
No. What I mean is that you are an individual with a unique perspective and a body that is interconnected but also uniquely experienced. And my goal is to get a sense of what it’s like to be you. What your current experience is like. What “feeling like something’s wrong” feels like. What “getting better” feels like.
And all of that information is located within story.
Your body tells us a story too. The story shows up in your emotions, in your physical sensations, in your behaviours (that might be performed automatically or unconsciously), in your thoughts, in your energy, and in the palpation of your body.
No two cases of rheumatoid arthritis are the same. They may have similar presentations in some ways (enough to fit the category in the medical textbooks), but the two cases of rheumatoid arthritis in two separate people differ in more way than they are the same.
And that is important.
We’re so used to 15 minute insurance-covered visits where we’re given a quick diagnosis and a simple solution. We’re conditioned to believe that that’s all there is to health and that the doctors and scientists and researchers know pretty much everything there is to know about the human body and human experience.
And that if we don’t know about something, it means that it doesn’t exist.
When we’re told “nothing is wrong” we are taught to accept it. And perhaps conclude that something is wrong with us instead.
When we’re told that we have something wrong and the solution is in a pill, we are taught to accept that too. And perhaps conclude that something is wrong with our bodies.
But, you know what a story does?
It connects the dots.
It locates a relevant beginning, and weaves together the characters, themes, plot lines, conflicts, heroes, and myths that captivate us and teach us about the world.
A story combines your indigestion, mental health, microbiome, and your childhood trauma.
A story tells me about your shame, your skin inflammation, your anxiety, and your divorce.
Maybe you don’t have a disease, even if you’ve been given a diagnosis.
She told me that lately, all the children she works with have a label. “Meredith can’t attend your online class because it’s her first day of school and she can’t handle more than two things because of her anxiety”, one mother wrote in an email as she backed out of a private class my friend had created by special request.
“Everyone is nervous on their first day of school”, my friend remarked, as she recounted the story to me.
“I need everyone’s microphones muted”, a 10-year old student exclaimed during an online class, “I have sensory overwhelm and attention deficit disorder and can’t handle background noise”.
My friend spent three years teaching in a rural school at the edge of a volcano in Guatemala. She worked in a private girls’ school in Colombia. And she taught grade 1 at an outdoor jungle school on the Pacific Coast of Mexico. “I’m not used to these North American kids”, she reflected.
“I wonder what diagnoses we’d have gotten in university?” I mused. I remember our Revolutionary Wall–pictures of Noam Chomsky, Victor Jara and Ghandi plastered on the wall that welcomed us into the entrance of our dirty apartment.
That year we’d worn our sweaters backward because it “felt right” to rest your chin on your hood, stopped washing our hair to “let the oils moisturize our roots”, and spent a week on a 1000-piece puzzle instead of going to class.
It was our last year. We were done.
My other friend was diagnosed with cancer, which would soon turn terminal. I was suffering from some sort of unacknowledged eating disorder–there were no body positivity Instagram feeds at the time. I could have used some.
It was a painful year.
For those and many more reasons, I’m sure, I was depressed.
I remember at some point during that year heading to a walk-in clinic because I was gaining weight, depressed, exhausted and completely shutdown. The walk-in clinic doctor told me “it wasn’t my thyroid” and to “eat less” so that I would lose weight.
I never got a diagnosis.
I was never offered an antidepressant.
I remember feeling hopeless. Desperate for an answer, but most of all, a solution.
If she had offered me an antidepressant, I’m certain I would have taken it. In fact, I did end up taking one about a year later for a brief period when living in Colombia (before the side effects made me stop).
I escaped a label.
My journey forked in the road and I took the one less traveled that led me towards naturopathic medicine.
Before that, though, I saw my own natural doctor who listened to me and put together the puzzle of my symptoms (who knew that skipping class to put together our 1000-piece puzzle would figuratively prepare me for my future career).
Rather than diagnose me, he listened to me and told me the underlying causes of my symptoms–not just what they were called.
And then, because we knew the cause, we also had a solution. And I soon felt better.
Of course, when I started naturopathic school, another 4-year full-time program with full days of classes (sometimes 10+ hours a day) and millions of exams and assignments, the underlying hormonal conditions that drove the original depressive episode I experienced at the end of my undergrad resurfaced.
I ended up seeing a fourth year naturopathic intern and she put me on something called adaptogens.
Adaptogens are class of plants. They support our Hypothalamic-Pituitary-Adrenal (HPA) response, which orchestrates the stress response. They are studied in rats who, when given adaptogens can perform longer on swim tests, producing less cortisol (our stress hormone) in the process.
These rats can tread water longer, without as much stress hormone and therefore, with less damage from stress. Depression is one of those side effects from the damage of psychosocial stress.
Stress leads to shutdown, inflammation and further hormonal imbalance, causing a wide variety of symptoms that seem disconnected but arise from the same source.
After all, isn’t depression, anxiety and burnout just us trying to keep our heads above water?
Oh man, did I ever wish I’d known about adaptogens in undergrad!
If I could have, I would have shouted about them from the rooftops, thrown bottles of them out of a plane, put them in the water supply.
I can’t do those things, but I can put many of my patients on them. Many of my patients suffering from depression and anxiety, caused by problems with their HPA axises, end up taking adaptogens.
I prescribe them when those I work with experience things like low mood, fatigue, sleep issues, inflammation (pain and swelling), hormone imbalances, particularly PMS or peri-menopause, sugar and salt cravings, delayed muscle recovery, tension, panic attacks and anxiety, dizziness and weakness, low motivation, and other oh-so-common symptoms often labelled as Major Depressive Disorder or other psychiatric illnesses.
Did I ever wish I’d known about adaptogens when I was in undergrad.
Instead I remember taking a crappy B vitamin complex from the local drugstore that a roommate’s mom gave me because I was on the birth control pill and “you need B vitamins on the birth control pill”. (Which is true: you need more vitamin B6 on the pill, but probably not one from a local drugstore multivitamin).
It didn’t do much.
I really really wish someone, a fairy godmother, the walk-in clinic physician, a man on the street, an article somewhere on the internet (like this one), had told me, “You have these symptoms because you are suffering from HPA axis dysfunction, as a result of significant psychosocial stress. This makes you suffer from the symptoms you’re dealing with, depression not being a condition of its own, but just another symptom of this condition.
“Adaptogenic herbs can help you get through this, as well as some important foundational lifestyle pieces that someone like a naturopathic doctor can help you with.
“There is a reason for your suffering. A context behind it. There is a cause we can identify.
“And, most importantly, there is a solution.”
But, I didn’t have anyone to tell me that.
I really wish someone had told me about adaptogens, but I haven’t ever wished that someone had diagnosed me with depression.
Now, a diagnosis can be extremely validating for some.
It can be lifesaving.
Medical intervention can also be really helpful for some people. But, like adaptogens (I should add), medications aren’t a one-size-fits-all solution.
We don’t know what causes depression and anxiety (likely many factors, HPA axis dysfunction being one of them), but we do know it’s not caused by a chemical brain imbalance.
And medications are designed to correct the brain imbalance that doesn’t exist, which is why they don’t work in everyone.
However, they do do something in some. Because, even though they don’t really solve the problem they’re supposed to (at least not in that simplistic way), they might be doing something else, which solves a problem in a few people.
The problem is, antidepressants make some people feel worse. In others they do nothing. And, in some of the people they do help, they don’t do enough. We’re still suffering.
And labels, while they can be helpful and lifesaving in some cases, can do damage in others.
Take my friend’s student with anxiety. What if her story of “I get stressed out on the first day of school because I have anxiety” turned into:
“I get stressed out on the first day of school because a lot of people do. It’s normal to feel nervous and anxious on the first day of school and want everything to go right.”
Now, of course, I don’t want to insinuate that anxiety isn’t a real thing. Of course it is!
There are many of us who suffer from anxiety disorders–a higher amount of anxiety than is common. Rather than first-day jitters, they might experience severe panic and complete dysfunction that make life miserable.
However, in the first example, the power is out of this student’s hands. It lies in her identity. In her dysfunction.
In her label.
In the second, it becomes a shared human experience, which she might be able to externalize and work with. Because it’s a common experience, she might find support, kinship, and understanding in those who experience the same.
Of course, I don’t know her case specifically. Maybe her diagnosis has helped her. Maybe her anxiety is well labelled and managed. Maybe she doesn’t need help. Maybe she is doing just fine.
All I know is, I wonder what I would have been diagnosed with, with my sweater on backwards, my hair full of grease, my body heavy like lead, a million puzzle pieces spewed all over the kitchen table in my dirty apartment with the revolutionary wall.
I have no idea what my diagnosis would have been, but I’m personally glad I never got one.
Instead, I wish I had had the permission to go through what I was going through.
I wish I’d had context for my suffering.
I wish I’d been given hope that things would get better.
I wish someone had empowered me through understanding the underlying causes of my symptoms and, of course,
“I followed X, Y, Z (controversial) diet, and my doctor said my blood is fine!”
Firstly, what do we think doctors are testing our blood for? Most standard blood tests look at cholesterol, check for anemia, and to see if our kidneys are failing or not.
If you’re lucky, your doctor might test your iron levels, B12, and thyroid function (using one hormone measure, TSH, which often fails to pick up cases of under-active, or autoimmune, thyroid).
Your doctor is likely not looking at inflammation levels, vitamin levels, hormone levels, insulin resistance, or delving into the nuances of your cholesterol levels. Standard blood tests do not provide a comprehensive analysis of your health status. Rather, they rule out the presence of serious disease.
Your blood tests are “fine” because the markers that might actually be negatively (or positively) impacted by your diet and lifestyle are simply not tested for.
Secondly, let’s challenge the notion of “fine”.
For most practitioners, “fine” means, “You don’t qualify for a diagnosis of X disease, which would justify the prescription of Y medication.”
I meet a lot of patients whose B12 levels aren’t “fine”, or whose thyroid levels are certainly not “fine”.
Sure, they are not deficient to the point where they have dementia (from low B12), or where they need thyroid hormone replacement medication, but their bodies are not working optimally.
If we dig a bit below the surface, we find that they are insulin resistant, they have elevated anti-thyroid antibodies, their B12 and iron levels are suboptimal, or their ovaries are not making progesterone.
Someone with these lab markers may not get a disease diagnosis from their medical doctor, and they may not need medication yet, but they’re not “fine”.
Oftentimes your blood tests are fine for decades—until they’re not fine.
This is a classic problem for those who are diagnosed with diabetes. I believe that for many patients, if we had done some exploration of their symptoms and blood 15 to 20 years earlier, we could have detected insulin resistance simmering below the surface of the conventional lab tests. (https://www.ncbi.nlm.nih.gov/pubmed/16627374)
Perhaps we could have prevented their diabetes, and subsequent cellular and metabolic damage, altogether.
I love it when we can do more in-depth lab testing based on your individual signs, symptoms, and risk factors. We take a full inventory of your lifestyle and health history and really dive into the nitty-gritty when it comes to preventing the diseases that your doctor looks for when ordering lab tests.
With the right approach, we might be able to keep those lab tests looking “fine”.