My Year of Living Ketogenically
 I review my adventurous year of living on the Low Carb High Fat Ketogenic Diet.
I review my adventurous year of living on the Low Carb High Fat Ketogenic Diet.
I’ve always had a sweet tooth.
I remember binging on Halloween candy as a kid, stuffing one tiny chocolate bar after another into my mouth, as fast as my little fingers could unwrap them, trapped in some kind of sugar-filled trance.
“Never get between Talia and her food!” My family would joke when my blood sugar would crash between meals and I’d rage towards the fridge for a snack to keep me sane.
I remember digging into the little bags of cheese popcorn reserved for school lunches, finishing off one after another and then hiding the wrappers in their big Costco box so that it would look like it was still full, the way rebellious teens top up empty vodka bottles with water.
I can gain weight with the drop of a hat (but also put on muscle fairly easily), and it takes concentrated effort and dedication to take it off.
After a period of temporary stress and bagel-related weight gain, I decided to embark on a bit of experimentation. Work was getting busy and I wanted to supply my brain with constant energy without having to take snack breaks every few hours. Also enticed by anecdotes of shattered weight loss plateaus, I decided to “go Keto”.
I like experimenting with diet. Like many health-conscious people, finding the right nutrition regime for me has been a process. In my teens I started controlling portions and switching out white breads for whole grain rye and Jolly Ranchers for carrot sticks. In my early 20’s, I was vegetarian. I tried being vegan for a while before deciding it was a disaster for my health when I began to experience nutrient deficiencies, weight gain, and hormonal issues.
Later on, I followed my naturopathic school classmates to a modified Paleo diet (keeping in some gluten-free grains and legumes), then moved to a more traditional Paleo diet (taking out the grains and legumes), before going back to the modified version (which is probably the best eating style for me—more on that later).
For the most part, my diet is comprised of whole foods, with lots of vegetables, but in the Fall of 2016, when this all began, I was in a pretty Standard North American place when it came to food intake. At the time I was suffering from IBS, some issues related to subclinical PCOS, and fatigue. I was also starting to see some signs of impaired glucose control.I wasn’t feeling good and I was in need of a kind of reset of sorts.
I was interested in seeing how relying on ketone bodies for fuel would help my body, mental performance, and improve my blood glucose control and symptoms. I have a family history of type II diabetes and I wanted to do what I could to prevent insulin resistance and metabolic syndrome. Drastic times call for drastic measures, I thought.
Ergo, The Ketogenic Diet.
About the Diet:
The Classic Ketogenic Diet was first developed in the 1920’s to treat children with medication-resistant epilepsy.
When our brains are starved of glucose, their preferred fuel source (our brains use up 60% of the body’s glucose), the liver creates ketone bodies from stored or dietary fat that the brain can use as a substitute source of energy.
One of these ketone bodies, beta-hydroxybutyrate, is thought to be a particularly therapeutic molecule for the brain, conveying anti-convulsive benefits, thereby helping to reduce the incidence of seizures in children who don’t respond to medication.
However, the original Ketogenic diet is more extreme than the general health and weight loss-aimed diet we see described in recipe books these days. The Classic Ketogenic diet consists of about 90% of calories coming from fat. In order to achieve that, followers need to severely restrict their protein intake, and virtually eliminate all dietary sources of carbohydrate, which drastically limits their nutrition choices.
Since, the benefits of beta-hydroxybutyrate are being studied for other neurological disorders, such as Parkinson’s disease, dementia, migraine headaches and narcolepsy. It’s being looked at as a potential treatment for mental health conditions, like autism and depression, and metabolic disorders such as type II diabetes, and even to increase the efficacy of chemotherapy and radiation treatments in cancer. Other studies are looking at its role in improving cognitive function in mice and humans.
Some research shows that beta-hydroxybutyrate can expand lifespan by interacting with genes that slow aging. It is also shown to confer anti-inflammatory and antioxidant benefits.
In the 1970’s, Dr. Atkins responded to the high-carbohydrate, low-fat dogma of the nutrition world at the time, by bringing a modified Ketogenic diet into vogue. Restricting all forms of carbohydrates and encouraging a consumption of the still-vilified high-fat foods like bacon, eggs and cheese, Atkins affirmed that people could lose weight by eating fat, as long as they restricted carbohydrates at the same time.
The modern version of the Ketogenic Diet is slightly more health-conscious, promoting a higher intake of vegetables. The current diet restricts carbohydrates to under 20 to 50 grams per day, and encourages a high fat intake and a moderate protein intake, in order to encourage the body to turn to fat as its primary source of fuel. The current version of “Keto” is less strict than it’s initial epilepsy-treating incarnation, with anywhere from 60-85% of its calories coming from fat.
My Version of Keto:
I started the whole journey by tracking my food intake (using My Fitness Pal). My aim was to consume 20 grams of net carbs, or less, per day to push my body into using fat-turned-to-ketone bodies as a its primary fuel source.
Net carbs are calculated by subtracting dietary fibre from total grams of carbohydrates. For example, 1 cup of raw broccoli contains 6 grams of carbs. 2.5 of those are fibre. Therefore, the net carbs in broccoli are 3.5, which would count towards my net carb goal of 20 grams per day.
This isn’t easy. Take a look at any package of food you regularly consume. 1 cup of cooked oatmeal contains 23 grams of net carbs: 3 grams over my entire daily allotment. Therefore all high-carb foods like grains, legumes, starchy nuts, all fruits, and some starchier vegetables, were off limits.
Many people opt to test their blood, breath or urine for ketone bodies to determine whether or not their bodies are in ketosis. I dabbled in this, using the urinalysis strips in my clinic to test for urinary ketones. However, even though I was sticking to the diet, the strips would mostly turn up negative for ketones.
There are a few reasons why ketone strips may not be a reliable marker for ketosis. Firstly, the don’t test for beta-hydroxybutyrate, which is the main ketone body utilized by the brain, but acetoacetate, another ketone body produced in the liver.
Secondly, urinalysis strips only test for urine ketone spillover. They don’t necessarily reflect blood levels, and they won’t pick up the ketones that are being utilized as fuel by the body. If cells are absorbing all the ketones the liver produces, urine testing may not be positive.
The most accurate, albeit more expensive, method for testing ketone bodies is through a skin-prick test that analyzes blood levels of beta-hydroxybutyrate.
While I knew that the urine strips weren’t highly accurate, not having my state of ketosis validated was discouraging. I was often left in doubt over whether things were “working”. I wondered if there was some other mechanism going on. Was my body finding carbohydrates from someplace else? Did I have Small Intestinal Bacteria Overgrowth that was digesting my fibre and allowing me to absorb it somehow? Were my blood ketones being used up somewhere else (by the yeast in my gut, for instance)?
I did have signs of being in ketosis that I could watch for, however. When I avoid carbs, or fast for a few days, I start to develop a metallic taste on the tip of my tongue. It’s not a common sign of ketosis, a more common sign is a “nail polish” or “paint thinner” taste in the back of the throat, but still a symptom that some people report.
Keto Flu:
During the first few days of switching to Low Carb High Fat, I had to white knuckle through a phase realistically termed the “Keto or Low Carb Flu”. This horrible phenomenon is thought to be a result of the body switching from burning glucose as its primary fuel source to adapting to ketone body production. There is often a painful adjustment period for brains that have to learn how to rely on ketones for their main fuel source after a lifetime of glucose abundance.
It was nasty. I felt intense hunger and sugar cravings, nausea, dizziness, and weakness—it truly was a “flu”.
I knew that I had spent most, if not all, of my life as a sugar burner. Before Keto, I would crave food even just two hours after a full meal. I would often feel “hangry”: dizzy and shaky in between meals, and irritable if made to wait for food for too long. I had been existing between carb-dense meals, experiencing insanity-inducing reactive hypoglycemia between my regular sugar fixes.
The more I read about others’ experiences, the more I was assured that the keto flu symptoms were actually a sign of my body healing. I was becoming adapted to other fuel sources, which was a good thing, I thought.
So, I muscled through and followed the online advice: I consumed more fat to provide more fuel to my brain, including medium chain triglyceride (MCT) oil, which is quickly absorbed by the lymphatic system and turned into ketones by the liver, and I consumed electrolytes, which are more rapidly excreted from the bodies of low carb dieters.
For some people, Keto flu can last for days, for others it lasts weeks. For me, the Keto flu thankfully only lasted two days, after which my body began to adjust and my cravings for sugar went down. I began to feel more energy, which felt encouraging.
Daily Meal Plan:
 For breakfast, I would typically eat a high-fat smoothie containing coconut milk yogurt, gelatin, and avocado, and topped with pumpkin seeds and cacao. Sometimes I’d make fat bombs or homemade unsweetened chocolate.
For breakfast, I would typically eat a high-fat smoothie containing coconut milk yogurt, gelatin, and avocado, and topped with pumpkin seeds and cacao. Sometimes I’d make fat bombs or homemade unsweetened chocolate.
I’d have my second meal of the day in the mid-afternoon, around 2 to 3 pm, for which I’d consume a few cups of cruciferous vegetables, like broccoli or cabbage, with a fatty cut of meat like ground beef, chicken thighs, or salmon, all topped with liberal amounts of fat from coconut, olives, avocados, or grass-fed ghee. I made a lot of batch-cooked grain-free curries and stews.
If I had a third meal or snack in the day, it would be another serving of fat: a handful of macadamia nuts or a hunk of creamed coconut.
Eating this way made me feel like Obama and his grey suits—I didn’t have to plan my meals too carefully. All I had to do was eat fat. My food was so calorie dense and my blood sugar so stable that I didn’t need to eat often. This meant that I didn’t need to worry about bringing food with me everywhere I went; one meal could satiate me for half the day. Hunger was never an emergency situation, as it had been in the past. Hunger would come on very slowly, and it would never be “hanger”; my already low blood sugar had nowhere to dip to. If I needed more food, I could always wait until I got home to eat.
More Benefits:
Within a few days, my PCOS- related cystic acne cleared. I also felt slimmer as some water retention deflated. This felt good. Our body stores carbohydrate in the form of glycogen in the liver and muscles. Glycogen stores retain water.
When glycogen stores are used up, a rapid 5 or more pound drop in weight can occur. This is the “water weight” that people talk about losing when they first begin some kind of nutrition plan.
It’s also common to notice a drop in water weight from a decrease in inflammation, when embarking on a new eating plan. I know that I am sensitive to certain carbs and dairy and, because those things were out of my diet overall (although Keto can certainly include high-fat dairy products for those who can tolerate them), the water retention caused by chronic inflammation seemed to clear.
Although it seems to attract people primarily for its hip-slimming potential, the Ketogenic diet probably does not cause weight loss in and of itself. Instead, the diet encourages a passive reduction in calories by stabilizing blood sugar and insulin levels, while promoting the intake of highly satiating foods containing protein and fat. Ketone bodies also have appetite-suppressing effects. Therefore, it’s probably a calorie deficit that causes the weight loss, rather than any specific biochemistry in the diet itself.
I didn’t lose much more weight than the water weight. However, my mood was brighter. I would wake up in the morning looking forward to the day, which often doesn’t happen in the winter. I felt more sustained energy throughout the day, and really enjoyed the decreased appetite, which led to more productivity.
I felt fine consuming two meals a day, able to get through hours of back-to-back patient visits without needing a snack or a break. It was actually incredible to need so few meals; it was like becoming another person, one no longer ruled by sugar cravings. I was like a camel, switching to stored fuel when the fat from my last meal had run out, and the transition was seamless. There was no wall to hit, and no hypoglcyemic crash to be seen.
I also noticed less bloating and digestive issues, probably from the lack of fermentation in my gut and the reduction in foods that tend to aggravate IBS, like certain vegetables, fruit, and legumes.
However, all was not roses on the Keto diet. While the first few months were dreamy, the longer I stayed on it the more I started to notice changes in my body that indicated the honeymoon period I was enjoying wasn’t going to last.
The Microbiome:
The research is in: human beings probably need 10 servings of fruits and vegetables a day (roughly 5 cups), or 800 g, a day to get the most heart disease, stroke and cancer-preventing benefits that diet can afford us. The International Journal of Epidemiology concluded that, if the correlations found in their February 2017 study were causal, almost 8 million lives might have been saved in 2013 if everyone in the world had simply consumed their fruits and veggies.
It’s one thing all diets, even the faddy ones, agree on—from the Paleo Peeps, to Plant-Based Hippies, to Raw Macrobiotic Sun Worshippers, to Whole Foods Michael Pollen Omnivores, to the dejected nagged-at husband pushing brusselsprouts around on his plate—fruit and vegetables are good for you. You should eat them. If you’re a typical North American, you should probably eat more than you’re eating. The health value of everything else we eat seems to be up for debate: red meat, saturated fat, soy, bread, coffee. The benefits of eating enough fruits and vegetables, however? There’s no contest.
It’s hard to pick one way in which fruits and vegetables are so health protective. It could be because of their high concentrations of micronutrients, reducing the risk of common nutrient deficiencies, like magnesium and vitamin C. It could be because, if you’re filling your body with a kilogram of fruits and vegetables a day, you probably aren’t scarfing down an entire medium-sized pizza and supersized orange pop as well—there just isn’t room. It could also be the antioxidants they contain that protect cells against free radical damage, protecting DNA. Or perhaps its the fermentable fibres present in fruits and vegetables that feed our invaluable microbiome.
The problem with keeping net carbs under 20 grams a day was that I needed to restrict my fruit and vegetable intake. I was eating no fruit at all, and staying away from the starchier veggies, like carrots and beets. I still stuck to my beloved leafy greens and crucifates, but even eating 2 to 3 cups of those guys a day would push me to the upper limits of my carbohydrate intake, which meant I couldn’t eat them as liberally as I had been.
Getting enough vegetables and (any) fruits on the keto diet is hard, if not impossible. This can impact our ability to get the micronutrients we need, but also enough fermentable fibres from vegetables like garlic, onions, yams, Jerusalem artichokes, and legumes, which provide food for our microbiome.
Feeding our gut bugs is important. They benefit us in numerous ways, from digesting out food, to calming inflammation, to fuelling gut cells by producing a short-chain fatty acid called butyrate. They help our immune systems function optimally. They produce neurotransmitters for our brains to work. They balance our stress responses and our circadian rhythms.
Jeff Leach, at the Human Microbiome Project speculates that the lack of dietary fibre in most low-carb diets may impact the health of the microbiome in negative ways by depriving the gut bacteria of their preferred food sources, as well as altering the acidity of the colon and intestines. He cites this article, in which obese subjects on a high-protein and low-carb diet had lower levels of butyrate in their bodies and intestines, likely due to decreased diversity in their guts.
There are, however, some studies that suggest that a Ketogenic diet can improve the microbiome in children with epilepsy, and autism, and some speculation by the researchers that that may be how the diets treat these conditions. However, since these studies are not done in “healthy” children, with an already healthy microbiota, it’s hard to extrapolate the findings to the healthy adult population.
Then there’s the fact that most studies that look at high fat diets and their impact on the microbiome are mostly done in rats. Of course, rats aren’t humans, despite there being relative genetic similarities. In these animal studies, researchers refer to “a high fat diet” when in fact they mean a high fat, high sugar diet. The sources of fat in these “high fat” mouse diets are often corn, margarine, or soy oil, which we know are highly inflammatory and offer few if any health benefits.
In other words, many studies on “high fat” diets are not looking at a relatively balanced Ketogenic diet that consists of vegetables, proteins, and healthy sources of fats from avocados, coconut, fish, olives, nuts and seeds and grass-fed meats.
Context is important as well. Is it the high fat diet that causes a reduction in gut diversity or the absence of fibre? This one mouse study showed that simply providing the mice with fibre in addition to their high fat diets decreased their risk of obesity.
I felt that my gut initially improved in the first few months on Keto: the diet was low in foods that aggravate me: namely refined carbs, sugar, gluten and dairy, as well as some of the fermentable fibres that can aggravate IBS. However, it never fully healed. After a few months, I started to notice the symptoms of bloating and digestive irregularities coming back.
Candida, a yeast that resides in the gut and can overgrow in the intestines in some people, especially the immunocompromised, causing symptoms of fatigue, IBS, and weight gain, among a variety of other symptoms, can survive on ketone bodies. Yeasts have mitochondria of their own. Some species of gut bacteria can consume protein, bile salts and even fats.
Contrary to what many claim, a Ketogenic diet doesn’t necessarily “starve out” the bad gut bugs. Combined with the lack of fibre to feed the beneficial gut bacteria and promote more bacterial diversity, a prolonged Ketogenic diet may be a recipe for gut dysbiosis.
Hormones:
Throughout my year spent in ketosis, I definitely noticed an improvement in my insulin signalling and glucose control, especially in the first few months. Looking at my blood work in March, after about a year of the Ketogenic diet (and then having been off it for a few months), my fasting insulin was very low and fasting blood glucose levels were in the low-optimal range. HOMA-IR, a calculation that is used as a marker of insulin resistance, was also low, indicating good insulin sensitivity.
I personally believe that this means that my risk for getting metabolic syndrome or type II diabetes is low, as long as I maintain this level of insulin sensitivity by watching the glycemic load of my diet and my stress levels.
The metabolic flexibility awarded to me from my year in ketosis also proved to be invaluable. Now, I no longer fear fasting and I can survive on other fuel sources besides sugar. My brain knows how to tap into stored and dietary fat more efficiently, and use those for energy. Even when not following any sort of low-carb diet, I noticed that I could survive between meals while travelling in Southeast Asia for two months, whereas normally I would have had to exist on unhealthy, sugary snacks.
However, after a few months on the diet, I began to notice a decline in my menstrual health. My cycles began to get longer, and soon I started missing periods. I noticed more hair falling out in the shower and more cystic acne developing on my chin. When I ran my blood estrogen and progesterone levels, I was surprised to see that their levels were very low.
We know that insulin, while often vilified as a “fat storage” hormone is actually responsible for storing everything, including nutrients. It also correlates with estrogen levels and the conversion of T4, one of our thyroid hormones, to its active friend, T3, which runs our metabolism. Insulin builds muscle, bone and brain cells. Very low insulin levels, in my case, were contributing to amenorrhea and a disruption in my sex hormones.
This wasn’t good.
While not quite the same as Intermittent Fasting (IF), Keto is often grouped into the same category because of its similar impact on blood glucose and insulin. The difference is that Intermittent Fasting induces ketosis through periodic food restriction, as opposed to carb restriction. Keto and IF often go hand in hand, however. The reduced hunger and high-nutrient density of the foods eaten on a Ketogenic diet often lend well to practicing intermittent fasting. It did in my case—I was only eating two main meals a day.
I always found it interesting, however, that most proponents of intermittent fasting are men. The male body appears to thrive in the fasted state, getting a boost of growth hormone and norepinephrine, both of which provide men with energy, motivation, and an improved sense of well-being.
This hormonal change may be a remnant of our ancestral hunter-gatherer days where it would be an advantage to feel motivated and energized to go out and hunt during periods of food scarcity.
I don’t think female bodies experience exactly the same effect. Some preliminary animal research tends to suggest that as well.
A few rat studies indicate that fasting may impair female insulin sensitivity, and induce amenorrhea, or missed periods. Female bodies rely on a consistent influx of calories and carbohydrates to stimulate insulin, which plays a role in stimulating thyroid hormones and estrogen, to continue to ovulate. Another study showed that fasting tended to “masculinize” female rats, lowering their female hormones, and increasing their levels of androgens, the male sex hormones, like testosterone.
Of course, these studies were done on fasted rats, which cannot be fully translated to the effects of Intermittent Fasting and Ketogenic diets on women. However, some of these findings did validate my experience, which certainly wasn’t being validated in the podcasts and blog posts I was exposed to, largely written and followed by men.
I did experience positive hormonal effects: the increased insulin sensitivity and lowered blood glucose. However, I was not happy about my irregular cycles and estrogen deficiency.
Therefore, I decided to increase my carbohydrate intake, returning to a more moderate Paleo diet that consists of some fruit, starchier vegetables and legumes. After a few months, my periods returned to normal, my skin cleared up, my hair stopped falling out, and my thyroid hormones, estrogen and progesterone levels all returned to their optimal ranges.
I have still have low fasting insulin levels, suggesting that the Ketogenic diet did help to reset my insulin sensitivity and that this effect may be lasting.
Metabolic Health:
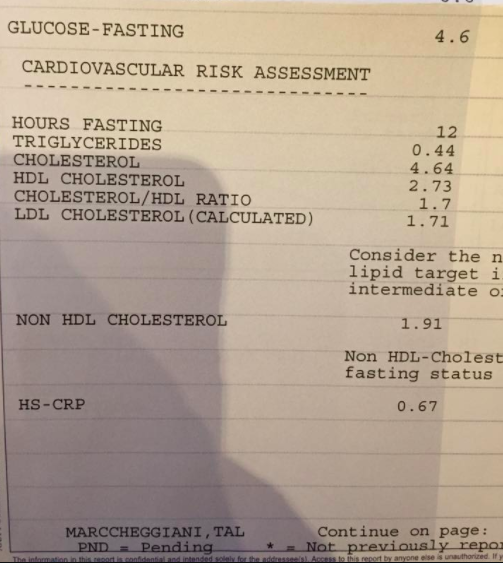 After a year of doing the Ketogenic diet, and then a few months of returning to a moderate-carb paleo diet, I tested my cholesterol levels and inflammatory markers. My HDL cholesterol (the “good” cholesterol, to put it very simply) was high, my triglycerides (a risk factor for heart disease) were very low, and my LDL cholesterol (the “bad” cholesterol that statin drugs target) was also low. My inflammatory markers: C-Reactive Protein (CRP) and erythrocyte sedimentation rate (ESR), were also low.
After a year of doing the Ketogenic diet, and then a few months of returning to a moderate-carb paleo diet, I tested my cholesterol levels and inflammatory markers. My HDL cholesterol (the “good” cholesterol, to put it very simply) was high, my triglycerides (a risk factor for heart disease) were very low, and my LDL cholesterol (the “bad” cholesterol that statin drugs target) was also low. My inflammatory markers: C-Reactive Protein (CRP) and erythrocyte sedimentation rate (ESR), were also low.
While it is typically the monounsaturated fats, like olive oils and avocados, that are associated with increased levels of the heart-protective HDL cholesterol, even saturated fats from coconut oil can raise HDL. LDL is often lowered by these healthy monounsaturated fats, however saturated fats, even healthy ones, can raise LDL in certain individuals.
All else being equal, higher levels of LDL may not be as big of a problem as we think. Especially in the context of low risk factors, like low inflammation, absence of smoking and a healthy body weight. What’s more, the triglycerides and cholesterol/HDL ratio may be more important factors for determining heart disease risk. Further, assessing LDL particle size may also provide those concerned about their LDL levels with more information concerning their cardiovascular health. That being said, it is important to be aware that some of the fats present in a Ketogenic diet have the potential to raise blood levels of LDL in certain susceptible individuals, and that not everyone’s blood lipid results will look like mine.
Triglyceride levels are associated with liver function, and generally reflect dietary sugar, fructose and refined carbohydrate intake, rather than fat intake. Reducing refined dietary carbohydrates like white grains, flours and sugars is a good strategy for reducing triglyceride levels and reducing heart disease risk.
Some individuals can experience elevated levels of inflammation on a Ketogenic diet, depending on the quality of foods consumed. A Ketogenic diet low in fibre that fails to feed the microbiome; high in foods that a person may have an individualized sensitivity to (such as dairy, eggs, nuts or soy); or high in inflammatory fats like trans fats, and industrial oils like canola and corn oil, may all contribute to increased inflammation.
That being said, certain ketone bodies like beta-hydroxybutyrate may have anti-inflammatory properties. Many of the fats consumed in a mindful, whole foods Ketogenic diet, such as olives, avocados, seeds, salmon, and coconut, are also anti-inflammatory.
I found my blood markers a good indicator of the power of a high-fat, low-carb diet to, at least in my case, improve HDL cholesterol and lower triglycerides, fasting insulin and fasting glucose levels. Whether I needed an entire year in ketosis, or whether I even needed to actually enter ketosis to receive these benefits, isn’t clear. Perhaps I could have gotten the same results by moderately lowering my carb intake while increasing my dietary intake of healthy fats.
Modified Ketogenic Diets:
While I do think I benefitted from entering into ketosis, I would not necessarily recommend a Ketogenic diet to patients unless to achieve some sort of therapeutic goal, such as improved insulin resistance, or for adjunct cancer care, to reduce inflammation, or to improve severe depression, migraines, or narcolepsy.
However, there may be a benefit to cyclical Ketogenic diets for memory and cognition, and increased life span in mice. Cyclical Ketogenic diets involve entering ketosis on alternate weeks. On the other weeks, participants return to a normal, whole foods diet that contains higher amounts of carbohydrates. In this case, individuals gets the benefits of beta-hydroxybutyrate production and increased metabolic flexibility on their weeks on, while also being able to eat a high amount of fermentable carbs and fibres on their weeks off, essentially getting the best of both worlds.
Adding medium chain triglycerides to food may also confer health benefits, similar to being on a Ketogenic diet. One study showed that adding MCT oil to a high-carb breakfast (pasta), reduced appetite in men. This is likely because, after burning through the glucose in the pasta, the men’s brains were able to access the ketone bodies that were made readily available by burning the MCT oil. This kept their brains fuelled and their bodies satiated for longer.
The men eating pasta and MCT oil in the study had a ketone blood level of 0.3, which is similar to that obtained from a diet that derives 10% of its calories from carbohydrates, which is an essentially a very low-carb, if not Ketogenic, diet. This may indicate that simply adding MCT oil to a moderate to low-carbohydrate diet, may confer some of the benefits of having a slightly higher rate of circulating ketone bodies without having to follow a strict diet. Again, following this strategy, you can get the best of both worlds: consume a diet high in fibre, while also getting a steady flow of ketone bodies to the brain.
Other interesting areas of research are the use of supplemental, or exogenous, ketones for therapeutic use, however the area is new and not something I currently recommend in my practice (although this may change when more research begins to emerge and better supplements enter the market).
My Plan Moving Forward?
I’m happy that I gave the Ketogenic diet a try, but now I’m back to my more modified Paleo diet, aimed at promoting gut health, optimizing my micronutrient intake, regulating hormones, and supporting my energy levels. I now consume berries and apples, legumes, starchier vegetables and lean proteins more often and aim to get 10 servings of fruits and vegetables a day, with 8 to 9 of servings coming from vegetables, as opposed to fruit.
I currently start my day with a smoothie with berries, an avocado, spinach and protein powder. For lunch I have some sort of protein, fat, and tons of veggies. I eat more often than when I was in ketosis: about 3 meals a day with a vegetable and fat as a snack, or no snack at all in between, depending on my schedule.
My total daily carbohydrate intake falls around 100 grams a day with a net carb intake between 50 to 70 grams a day, depending on the fibre content of the vegetables, seeds, and legumes I’ve eaten that day. I try to get upwards of 30 grams of dietary fibre per day.
I avoid all sugar, including sweeter fruits like tropical fruits, and dried fruits, like dates. I especially stay away from refined sugars, even “natural” coconut sugars and agave. I avoid processed carbohydrates and flours. I mostly avoid grains, except when travelling or visiting someone’s house, getting my carbs from starchy vegetables and tubers, legumes and berries. I continue to avoid dairy (which I’m sensitive to), gluten, and processed industrial oils like canola, corn, and soy oil.
Right now, rather than focussing on macronutrient ratios, I’m directing my food intake towards obtaining the Recommended Daily Allowances of the micronutrients that run all of our cellular reactions, and the fibres that feed a healthy gut microbiota. I use an app called Cronometer to track this.
I definitely eat more fat than before, adding MCT oil to my morning smoothie, especially on days when I need to stay full and focused for longer. I also aim to do at least 12 hours of fasting a day, trying to get in 16-18 hour fasts where I can, ending dinner at 4pm, for example. I no longer do regular long bouts of Intermittent Fasting, particularly not when I’m feeling stressed and burnt out.
Would I Recommend the Ketogenic Diet to Patients?
One of the main tenants of Naturopathic Medicine is “Do no harm”. While it may seem like making diet and lifestyle recommendations are relatively benign therapies, I believe that they do have the potential to do physical and psychological harm, particularly if they are strict recommendations.
Following a strict diet may have health benefits, but it also may isolate us from friends and family, frustrate us and restrict our intake of certain nutrients, like fibre, vitamins and minerals. This is one of the reasons I do not ever advocate a Vegan diet, although if patients are following one already, I believe in guiding them to optimize their nutrient intake.
Furthermore, at least in my personal experience, the cure was stronger than the disease. I probably didn’t need to do the Ketogenic diet for so long; this was evidenced by the hormonal imbalances that I began to experience towards the end of my year on the diet.
However, particularly for patients who are suffering from metabolic syndrome, type II diabetes and insulin resistance or PCOS, there may be some powerful benefits to entering ketosis in order to dramatically reverse metabolic dysfunction. In this case, a modified regime combining Intermittent Fasting and cyclical Ketogenic diets could be beneficial.
Of course, it all depends on where patients are at in their nutrition journeys. Sometimes I meet patients who require, and respond well to, more heroic lifestyle interventions. Other times I meet patients relying on several sugary treats a day to get them through. In these cases, simply tweaking their diet in small ways, using baby steps may also have powerful disease-risk-reversing effects.
For more, catch the video.